Introduction to oncopathology Principles of classification of tumors. Morphological characteristics of benign and malignant epithelial tumors. Morphological classification of tumors
Morphological classification of tumors
The General Nomenclature of Human Tumors (WHO in 1959) was based on histogenetic and localization principles, taking into account the clinical course of the disease. Subsequently, an expanded nomenclature of tumors was created, which formed the basis of the WHO classifications of tumors.
Within the framework of the WHO classifications, there is a classification according to the TNM system (Tumor - a tumor, Nodulus - metastases to the lymph nodes, Metastasis - hematogenous metastases). This classification is important for the prognosis and treatment appointments.
Principles of morphological classification
Based on the histogenetic principle, 7 groups of tumors were identified.
1. Epithelial tumors without specific localization (organ-nonspecific).
2. Tumors of exo- and endocrine glands, as well as epithelial integuments (organ-specific).
3. Mesenchymal tumors.
4. Tumors of melanin-forming tissue.
5. Tumors nervous system and membranes of the brain.
6. Tumors of the blood system.
7. Teratomas.
The division of epithelial tumors into organ-nonspecific and organ-specific is not justified, because for most tumors, there are organ-specific markers, which is important in the morphological diagnosis of tumors.
Epithelial tumors without specific localization
These tumors, which develop from squamous or glandular epithelium that do not perform a specific function, are divided into benign and malignant.
benign tumors
This group includes papilloma and adenoma.
Papilloma. Tumor of squamous or transitional epithelium. It has a papillary appearance (reminiscent of cauliflower), built from cells of the integumentary epithelium, the number of layers is increased. The stroma is well expressed and grows together with the epithelium.
In the papilloma, the properties of the epithelium are preserved: polarity, complexity, basement membrane. Localized on the skin, oral mucosa, esophagus, vocal cords, renal pelvis, ureters, Bladder.
Adenoma. Tumor from prismatic and glandular epithelium. It occurs on mucous membranes lined with prismatic epithelium and in glandular organs. Mucosal adenomas protruding above the surface in the form of a polyp are called adenomatous (glandular) polyps. If the stroma is strongly developed in the adenoma, then they speak of fibroadenoma. Distinguish alveolar, trabecular, papillary adenoma. If cavities are formed in the adenoma, then they speak of a cystadenoma.
Malignant tumors
A malignant tumor of the epithelium - cancer. Developing from poorly differentiated epithelial cells.
Microscopic forms of cancer
"Cancer in Place"(carcinomainsitu) - without infiltrating growth, with pronounced cellular atypia. The basal memboana does not germinate.
Squamous cell (epidermal) cancer. It develops in the skin and mucous membranes covered with squamous epithelium.
Two options:
1. Keratinizing cancer - cancerous pearls are formed.
2. Non-keratinizing squamous cell carcinoma - low differentiation and without keratinization.
Adenocarcinoma (glandular cancer). It develops from the prismatic epithelium lining the mucous membranes, and the epithelium of the glands.
Depending on the degree of differentiation, there are:
1. Highly differentiated;
2. Moderately differentiated;
3. Poorly differentiated adenocarcinoma.
Mucous (colloidal) cancer. Tumor cells produce a lot of mucus. Mucous carcinoma is one of the forms of poorly differentiated adenocarcinoma.
Solid cancer. A form of low-grade cancer. Has a trabecular structure.
Small cell cancer. A form of low-grade cancer. Made up of lymphocyte-like cells.
Fibrous cancer (skirr). It is built from a small number of atypical cells and a highly developed stroma.
medullary cancer. Poorly differentiated cancer, characterized by the predominance of the parenchyma over the stroma.
Tumors of exo- and endocrine glands, as well as epithelial integuments
The cells of these tumors, while retaining the functional and morphological features of the organs from which they develop, are found in epithelial integuments, exo- and endocrine glands.
Tumors of exocrine glands and epithelial integuments
Liver
Hepatocellular adenoma. A benign tumor arising from hepatocytes forms trabeculae.
Hepatocellular (hepatocellular) cancer. Built from atypical hepatocytes. May grow as one or more nodes. Has trabeculae or tubular structures. The stroma is weakly expressed, there are many vessels.
kidneys .
Adenoma. Benign tumor, tubular or trabecular structure. Distinguish:
1. Dark cell;
2. Clear cell (hypernephroid);
3. Acidophilic adenoma.
Renal cell (hypernephroid) cancer. Malignant tumor. Growth through the veins and early hematogenous metastases to the lungs, bones, liver, and opposite kidney are characteristic.
Allocate microscopic forms:
1. Clear cell;
2. Granular cell;
3. glandular;
4. Sarcomatous;
5. Mixed cell.
Nephroblastoma (embryonic kidney cancer, Wilms tumor). A malignant tumor of a mixed structure, consists of epithelial cells that form solid and tubular structures, and striated muscles, fatty tissue, cartilage, and blood vessels. Occurs in children.
Breast
Tumors are very diverse, often developing against the background of dyshormonal dysplasia.
Fibroadenoma. A benign tumor of the glandular epithelium with a highly developed stroma. Distinguish:
1. Pericanalicular;
2. Intracanalicular;
3. Mixed;
4. Leaf-shaped (phylloidal) tumor.
Mammary cancer.
Presented:
Non-infiltrating lobular and intraductal carcinoma.
· Paget's disease.
Non-infiltrating lobular carcinoma (lobular "cancer in situ"). R asthete within the lobule, has glandular or solid variants.
Non-infiltrating intraductal carcinoma (ductal "cancer in situ"). It can be papillary, cribriform and acneiform (gummy carcinoma). Grows within the duct, often undergoes necrosis, calicinates are possible.
Paget's disease. It develops from the epidermis or epithelial cells of large ducts. Large light cells (Paget cells) are formed in the basal and middle layers of the epidermis. The tumor is localized in the area of the nipple and areola.
All of the listed forms of breast cancer with progression turn into infiltrating ductal and lobular breast cancer.
Uterus
Epithelial tumors are represented by destructive hydatidiform mole and chorionepithelioma.
Destructive (malignant) hydatidiform mole. It is represented by large chorionic villi growing into the walls of the veins of the uterus and small pelvis. The villi are dominated by syncytial cells.
Chorioepithelioma (chorioncarcinoma). A malignant tumor of the trophoblast that develops from the remnants of the placenta. It consists of elements of cyto- and syncytiotrophoblast. The stroma of the tumor is absent, the vessels look like cavities in which tumor cells float. Hematogenous metastases are characteristic. The tumor is hormonally active, simulating pregnancy. Sometimes there are ectopic chorionepitheliomas: in the mediastinum, testicles in men, bladder, ovary in women.
Leather
Syringoadenoma. Benign tumor of the epithelium of the ducts of the sweat glands.
Hydradenoma. A benign tumor of the secretory epithelium of the sweat glands that forms papillae.
Trichoepithelioma. A benign tumor from the epithelium of the hair follicle, cysts filled with horny substance are typical.
Basal cell carcinoma (basalioma). The tumor develops from the basal cells of the epidermis, the cells are arranged in strands or nests. The tumor grows radially, destroying the adjacent tissue, but does not give metastases, recurs.
Malignant tumors of skin derivatives are represented by sweat cancer, sebaceous glands and hair follicles.
Tumors of the endocrine glands Table 3. Tumors of the endocrine glands
ovaries
Tumors can develop from the epithelium, stroma, sex cord and germ cell tissue; they can be benign and malignant.
Serous cystadenoma. A benign epithelial tumor that looks like a cyst is filled with serous fluid. Sometimes in cysts papillary proliferation of the epithelium is possible.
Mucinous cystadenoma. Benign epithelial tumor. The cysts are lined with prismatic epithelium, with mucus in the cavity. Sometimes the lining epithelium forms papillae. In case of rupture of the cyst, implantation of cyst cells along the peritoneum is also possible.
Serous cystadenocarcinoma. Malignant epithelial tumor, has a papillary structure. Characterized by implantation metastases in the peritoneum.
Pseudomucinous cystic carcinoma. A malignant epithelial tumor that forms solid, glandular, cribriform structures.
Tekoma. Benign tumor from the stroma of the sex cord. The structure may resemble a fibroma. This variant of the tumor is usually hormonally inactive.
Malignant thecoma. It is characterized by pronounced polymorphism and atypia of cells, resembles sarcoma, and is hormonally inactive.
Granulosa cell tumor (folliculoma). Benign tumor of the sex cord stroma. Grows from granulosa. The tumor is hormonally active and produces estrogens.
Malignant granulosa cell tumor. It is characterized by high cell polymorphism, rapid growth and metastases.
Dysgerminoma. A malignant tumor formed from the cells of the rudiment of the male gonad resembles a seminoma; lymphocytes are found in the stroma.
testicles
Distinguish:
1. Germinogenic tumors;
2. Tumors from cells of the gonadal stroma;
3. Tumors arising from the membranes of the testis and appendages;
4. Tumors developing from germ cells and cells of the gonadal stroma.
Seminoma (dysgerminoma). A malignant tumor built from atypical germ cell epithelium. Occurs most often. Metastasizes early.
Leydig cell tumor (leidigoma). It develops from glandulocytes - cells of the gonadal stroma, benign, hormonally active.
Sertoli cell tumor. A benign tumor of sustentocytes, hormonally active, causes premature puberty in children.
Tumors from germ cells and cells of the gonadal stroma (gonadoblastoma). They develop from seminoma-type cells and cells resembling sustentocytes and granulosa cells. The germ cell component metastasizes.
THYROID. Tumors can arise from cells A, B, C, benign and malignant.
Follicular adenoma. Arises from cells A and B, in structure resembles the thyroid gland.
Solid adenoma. It develops from C cells that produce calcitonin. Forms papillae. The presence of the latter is an unfavorable sign in relation to malignancy.
Cancer thyroid gland
1. Follicular cancer. Built from atypical follicular cells. Gives hematogenous metastases to the lungs and bones.
2. papillary cancer. The most common malignant tumor of the thyroid gland. It has a papillary structure.
3. Solid (medullary) cancer. It develops from C cells that produce calcitonin. In this cancer, amyloid is detected in the stroma, which is formed by tumor cells of the APUD system.
4. undifferentiated cancer.
Parathyroid glands
Adenoma. G rmonally active. Accompanied by hyperparathyroidism, which causes the development of fibrous osteodystrophy.
Cancer of the parathyroid glands. IN occurs rarely.
adrenal glands
Tumors arise from the cortical and medulla layers. They can be benign and malignant.
Benign tumors of the cortical layer.
Clear cell adrenocortical adenoma. Produces aldosterone and causes Kohn's syndrome. This adenoma is also called an aldosteroma.
Dark cell adrenocortical adenoma. Produces androgens (androsteroma), so there are signs of virilism, less often Cushing's syndrome.
Mixed adrenocortical adenoma orthosteroma). Manifested by hypercortisolism (Cushing's syndrome).
Glomerular cell adenoma. Manifested by increased production of mineralocorticoids.
Malignant tumor of the adrenal cortex.
adrenocortical cancer. Built from atypical polymorphic cells, gives hematogenous metastasis.
Benign tumor of the brain.
Pheochromocytoma. A hormonally active tumor secretes catecholamines, which leads to an increase in blood pressure.
Malignant tumor of the adrenal medulla.
Malignant pheochromocytoma. It is characterized by pronounced cellular atypia, usually hormonally inactive.
Thymus
Tumors arising from cortical and medullary cells are benign and malignant. Clinically, they are asymptomatic or cause myasthenia gravis, immunodeficiency syndromes, and autoimmune diseases.
There are 4 types of thymomas.
1. Cortical cell thymoma;
2. Medullary cell thymoma;
3. Mixed cell thymoma;
4. Granulomatous thymoma.
Pituitary
Adenoma. Histologically distinguish chromophobic, eosinophilic, basophilic adenomas. ABOUT They do not have hormonal activity. According to hormonal activity, adenomas are distinguished:
1. Somatotropic;
2. Prolactin;
3. Adenoma from cells secreting ACTH;
4. Adenoma secreting thyroid-stimulating hormone;
5. Adenoma from cells secreting follicle-stimulating hormone.
Cancer. A malignant analogue of pituitary adenomas.
epiphysis
Pinealoma. Benign tumor of glandular epithelium and neuroglia; causes metabolic and hormonal disorders.
Pancreas
Tumors of the islet apparatus of the pancreas are referred to as tumors of the APUD system (apudomas). Distinguish:
Insuloma. It develops from the B-cells of the islet apparatus. The structure resembles a trabecular or tubular adenoma. Hormonally active, cells produce a large number of insulin, which leads to the development of hypoglycemic syndrome.
Gastrinoma. Develops from G-cells. It happens multiple. The structure resembles a trabecular adenoma. It is hormonally active, produces gastrin, which leads to the development of the Zollinger-Ellison syndrome.
Glucagonoma. From A cells that synthesize glucagon. The structure looks like a trabecular adenoma. It causes hyperglycemia and the development of diabetes mellitus.
Vipoma. It develops from D 1 -cells that produce a hormone such as vasoactive intestinal polypeptide hormone (VIP). The structure is solid-trabecular, causes hypokalemia and dehydration.
Serotonin. It arises from E c cells that produce 5-hydroxytryptamine. Has a solid trabecular structure, causes carcinoid syndrome.
Somatostatinoma. D-cell adenoma. The structure resembles a solid trabecular adenoma; hypoinsulinemia, hypoglucagonemia, steatorrhea, achlorhydria are characteristic.
All of these tumors have malignant counterparts that may be hormonally active.
Gastrointestinal tract
Carcinoid. It develops in the mucosa of the gastrointestinal tract from enterochromaffin cells (Kulchitsky cells), which produce biogenic amines (serotonin). In structure, it resembles a solid trabecular adenoma, gives an argentaffin and chromaffin reaction. Patients develop carcinoid syndrome.
Benign tumors are characterized by slow growth, delimited from the surrounding tissues by a capsule, tumor cells do not spread throughout the body with blood or lymph flow, that is, they do not metastasize. A benign tumor does not affect general condition the patient until it begins to compress the surrounding tissues and organs. nerve trunks, blood vessels, causing a violation of their function. A benign tumor can be radically surgically removed. Benign tumors are divided into epithelial, non-epithelial, and inflammatory.
Epithelial tumors include::
- Papilloma- a tumor, the basis of which is connective tissue, covered with epithelium. It occurs on the skin, mucous membranes of the gastrointestinal tract, bladder, larynx. Papillomas may be various shapes(in the form of villi, cauliflower, warts, papillae). Papillomas during trauma can bleed, can disrupt the function of the organ and turn into a malignant tumor. They can be congenital and acquired. One or another type of papillomas occurs in almost every person. Intensive immunological and virological studies in recent decades have revealed a large group of human papillomaviruses. The spread of papillomas is considered as a kind of reactive proliferation of the epidermis in response to viral exposure in conditions of reduced immunity.
- Adenoma- develops from the glands and has the structure of the organ from which it develops (prostate adenoma, thyroid adenoma). The epithelium of the adenoma secretes a secret characteristic of the main glandular tissue from which the tumor was formed.
- Dermoid (dermoid cyst) is a tumor that develops from the embryonic rudiments of the ectoderm. It consists of the skin and its appendages, so in its cavity there can be not only the epidermis, but also hair and fat.
Nonepithelial tumors - tumors of connective tissue origin:
- Fibroma- consists of fibrous connective tissue with a small number of blood vessels and elastic fibers. Fibromas can be single and multiple, soft and dense, they can be located wherever there is connective tissue (in the skin, subcutaneous adipose tissue, fascia, aponeurosis, nerve trunks, uterus). If other tissues are present in the tumor, then fibromyomas, fibrolipomas, fibroadenomas are formed. Fibroma on a narrow stalk is called polyp.
- Lipoma- a benign tumor of adipose tissue that has a capsule. It is located in the subcutaneous adipose tissue in the form of single or multiple nodes. Most often localized on the neck, back, forearm. The lipoma can be located more deeply. The tumor has a soft-elastic consistency and a lobed structure.
- Chondroma is a benign tumor of cartilage. Dense consistency, develops slowly.
- Osteoma is a tumor of mature bone tissue. It develops for a long time. In this case, there is no pain, and a palpable formation, in most cases, becomes the first sign of the disease.
Tumors of muscle, vascular and nervous tissue:
- myoma- benign tumor of muscle tissue;
- leiomyoma- a tumor of smooth muscle fibers;
- rhabdomyoma- swelling and striated muscles; The combination of muscle and connective tissue tumors is fibromyoma; more often fibroids develop in the uterus;
- angioma- a tumor that develops from blood vessels. Develop from blood vessels hemangiomas, from lymphatic - lymphangiomas. Often congenital;
- simple (capillary) hemangioma has the appearance of small pigmented spots of red or blue-red color, somewhat prominent above the surface of the skin. When pressed, the size of the tumor decreases. Sometimes the size of the tumor can be significant;
- cavernous angioma- looks like dark blue nodes or flat swelling, has a spongy structure with cavities filled with blood;
- branched angioma- consists of dilated tortuous vessels, translucent through the skin in the form of a pulsating swelling;
- neuroma- a tumor from the nervous tissue, often accompanied by severe pain;
- glioma- a tumor consisting of neuroglia of the brain tissue of the brain or spinal cord;
- ganglioneuroma- a tumor of the sympathetic nerves, can reach a large size.
mixed tumor- This is a neoplasm consisting of several tissues that have independent growth. They occur when there is a violation embryonic development. Mixed tumors are divided into two groups:
- simple mixed tumors - formed from two germ layers;
- complex tumors - from three germ layers.
Simple mixed tumors more common in the parotid or other salivary glands, in the mammary gland. They consist of cartilage, adipose, mucous tissue, epithelial cells and glandular formations. Surrounded by a capsule, not soldered to adjacent tissues, grow slowly.
Complex mixed tumors are divided into teratoid and teratoma. Teratoid tumors resemble dermoid cysts, but their composition is more complex (hair, teeth, bone plates).
Teratoma are innate formations. More often located on the surface, in the region of the skull and coccygeal region. It contains parts of organs and whole organs.
See oncology
Saenko I. A.
Sources:
- Barykina N. V. Surgery / N. V. Barykina.- Rostov n / D: Phoenix, 2007.
- Barykina N.V. Nursing in surgery: textbook. allowance / N. V. Barykina, V. G. Zaryanskaya.- Ed. 14th. - Rostov n/a: Phoenix, 2013.
It should be noted that benign tumors can degenerate into malignant ones under the influence of various adverse external and internal influences.
Tumors with locally destructive growth occupy an intermediate position between benign and malignant tumors. Unlike benign tumors, they have signs of infiltrating growth. Unlike malignant tumors they do not metastasize.
TUMOR GROWTH OPTIONS
depending on growth rate distinguish between tumors fast And slowly growing(several weeks or months and many months or years).
Depending on the presence or absence of dissemination(from lat. dissemino-spread) tumors grow either with metastases (see next section), or without metastases .
Depending on the degree of differentiation of tumor cells There are two main types of tumor growth : 1) expansive and 2) infiltrating .
Expansive (pushing back) growth characteristic of benign tumors and some malignant (kidney cancer, fibrosarcoma). Intensively dividing, maturing cells provide slow growth swelling of itself, leading to retraction , exclusion of surrounding tissues.
Infiltrating (invasive) growth characteristic of most malignant tumors. Extremely rapidly dividing immature cells lead to rapid growth of a tumor capable of metastasizing (see next section), i.e. spread throughout the body and the formation outside the primary tumor of a different number of secondary foci of tumor growth in distant tissues and organs.
In relation to the lumen of a hollow organ, tumor growth can be: 1) exophytic(expansive tumor growth into the cavity of an organ, for example, into the cavity of the stomach, uterus) and 2) endophytic(infiltrating tumor growth inside the wall of a hollow organ).
21.4. PRE-BLASTOMA (PRE-CANCER) CONDITIONS
Under the term precancer, according to academician L.M. Shabad understood " pathological condition, characterized by a long-term coexistence of atrophic, dystrophic and proliferative processes, which precedes the development of a malignant tumor and in a large number of cases passes into it with increasing probability.
In fact, the term "precancer" refers to oaz-like, and not only preblastoma states of epithelial origin.
In particular, to precancerous conditions relate:
- chronic proliferative inflammatory processes and diseases, accompanied by phenomena of both intensive proliferation (growth of cellular and tissue structures), and dystrophy and atrophy (specific examples are chronic gastritis, stomach ulcers and duodenum, erosion of the cervix, etc.);
- hyperplastic processes and diseases accompanied by the development of foci of cellular hyperplasia, often glandular tissue, without the phenomena of tissue and cellular cataplasia ( concrete example can serve fibrocystic mastopathy and etc.);
- benign tumors(papillomas, adenomas, fibromas, lipomas, fibroids, osteomas, gliomas, nevi), which under the influence of various carcinogens can turn into malignant tumors (cancer in situ, cancer, adenocarcinoma, sarcoma, glioblastoma, melanoma, etc.).
Some precancerous conditions that have a hereditary predisposition are always maligned - these are the so-called obligate (mandatory) precancers. Others do not always turn into malignant tumors - these are the so-called facultative (optional) precancers.
Some precancerous conditions occur in tissues and organs. Contacts with external environment(mucous membranes of the eyes, digestive and respiratory tracts, skin). They are often accompanied by prolonged inflammation, characterized by the activation of proliferative, as well as dystrophic and atrophic processes.
Other precancerous conditions occur during internal organs not in direct contact with the external environment. They are usually not accompanied by a long inflammatory process.
21.5. BIOLOGICAL FEATURES OF MALIGNANT TUMORS
Unlike physiological and other pathological species tissue growth, the growth of malignant tumors is characterized by the following features.
Lack of control and autonomy of growth. This quality of tumor cells is associated with a complete or partial disruption of the diverse mechanisms of regulation of the process of their proliferation. Increased sensitivity to various factors growth. Reduced or even absent contact and other types of inhibition of division and maturation of these cells.
Infinity of growth. It is well known that normal (healthy) cells mature rapidly and in the course of their life have a genetically determined (limited) number of divisions and life expectancy. Back in 1961 L. Haytflick P.S. and Moorhead found that mammalian cells have a limited number of divisions (50-60). This phenomenon of a limited number of divisions is called cellular aging (Hayflick cell limit). Unlike healthy ones, malignant tumor cells do not have such a division limit, which is why their population is almost immortal. A clone of tumor cells, eternally young and incapable of maturation and aging, can live for decades (this phenomenon is called cell immortalization). Fast growth tumor is associated not only with an increase in the rate of cell division, but with the inhibition or lack of regulation of the inhibition of their proliferation, as well as with the activation of angiogenesis and microcirculation in the tumor. The latter depends on an increase in the amount and activity of some regulatory substances (angiogenin, a- and b-transforming growth factors, hepatocyte growth factor, interleukin-3,8, etc.) and a decrease in the amount and activity of others (angiostatin, interferons a- and b, heparinase, tissue inhibitor of metalloprotein h, thrombospondin).
Infiltrative (invasive) growth. Malignant tumors germinate not only the walls of blood vessels, but their surrounding tissues, destroying them. This property, as well as the ability of tumor cells to easily break away from neighboring cells, is associated with an increase in their enzymatic (proteolytic) activity and a decrease in the density (adhesion) of intercellular contacts.
Anaplasia (cataplasia). Under anaplasia(from the Greek. ana - a prefix meaning reverse action) return of cells and tissues to an undifferentiated state; at the same time they cease to perform specific functions cataplasia(from the Greek kata - downward movement and plasis - formation, formation) - partial or complete loss of tissue-specific features as a result of the appearance of poorly differentiated or undifferentiated cells. Allocate the following types tumor anaplasia.
· Morphological anaplasia. It can be both tissue and cellular.
Tissue anaplasia is manifested by an increase in the ratio: parenchyma volume / stroma volume, a decrease in the number of large vessels and an increase in the relative amount small vessels(capillary type), a decrease in the number of lymphatic capillaries and nerve endings.
Cellular anaplasia is manifested by rejuvenation (simplification) of cells, a return of their structure to the embryonic organization, cell polymorphism (an increase in size, the appearance of a shape that is not typical for a particular tissue), an increase in the number of multinucleated cells, an increase in the number of chromosomes, a change in the number, size, shape and structure nuclei, ribosomes, mitochondria, Golgi apparatus and other organelles, as well as changes in the structure of cell and subcellular membranes.
metabolic anaplasia. The severity of the latter usually corresponds to the degree of cell dedifferentiation and the growth rate of malignant tumors. The following manifestations of cataplasia are most characteristic of them:
Severe intracellular acidosis (due to the accumulation of lactate and other incompletely oxidized metabolic products resulting from the activation of the process of both anaerobic and aerobic glycolysis, especially after a load of glucose and even in the presence of oxygen);
Increase in the intracellular content of water, potassium, sodium, iron, zinc ions, etc.;
Quantitative and qualitative change synthesis of proteins in tumor tissues (an increase in anabolism and a decrease in protein catabolism, sometimes activation of the synthesis of embryonic proteins - a-fetoprotein, etc., a change in the enzymatic composition of cells (according to the enzymatic composition of the tumor cell closer friend to a friend than to normal cells), increased DNA synthesis;
A sharp increase in the use of glucose, amino acids by the tumor (“glucose and amino acid trap”), as well as vitamins, PAS and some other substances;
Immunological (antigenic) cataplasia. The antigenic composition of malignant tumors is distinctly different from normal tissues. In particular, the following types of tumor antigens can be found in them.
Tumor antigens induced by the action of various carcinogens. As a result of mutations caused by carcinogenic factors, tumor cells can synthesize proteins that have antigenic properties. They are strictly individual and differ in polymorphism depending on the type of carcinogens.
Antigens of viral tumors. When tumors are induced by the same virus, these antigens are the same for several tumors both in one individual and in different individuals.
Embryonic antigens - proteins (for example, a-fetoprotein, cancer-embryonic antigen, etc.) resulting from antigenic reversion.
Heteroorgan antigens. In some cases, especially with immunosuppression of insufficiency, tumors of some organs may contain antigens characteristic of other organs ( antigenic divergence).
Tumor tissue usually eludes the body's strict immune surveillance that is characteristic of healthy tissue. This may occur primarily as a result of:
Reducing tissue-specific and individual antigens while maintaining species-specific antigens (to the latter, each organism of the same species has immunological tolerance, i.e. tolerance, insensitivity);
- appearances embryonic antigens;
Masking of tumor antigens from immune surveillance, for example, as a result of the formation of blocking antibodies, coating of tumor cells with a fibrin film, or the development of immune suppression (secondary immunodeficiency).
functional cataplasia. It manifests itself as a clearly expressed change in the specific functions of cellular tissue structures. Functional activity of tumor cells in varying degrees may decrease, increase or pervert. For example, with tumors of the endocrine glands, an increase in the formation of a hormone or a decrease in its synthesis can be observed.
Metastasis, i.e. its spread and the formation of daughter tumors occurs in three ways:
Lymphogenically along the paths of lymph flow to regional lymph nodes,
through the interstitial fluid (metastasis to nearby organs),
perineurally
Hematogenous (metastasis to distant organs).
The hematogenous route of metastasis is the most dangerous, since in this case, daughter tumors can form in any organ, and often it is the presence of metastases that causes the patient to be inoperable, or they are not detected during the examination of the patient before surgery and subsequently cause a relapse of the disease. Tumor metastasis is inextricably linked with the mechanisms of invasion, since in order for tumor cells to enter the lymph, blood, or interstitial space, they must go through several barriers, in particular, through the extracellular matrix.
The following stages are distinguished: angiogenesis in a tumor invasion tumor cells detached from the primary tumor focus into the surrounding tissues, interstitial space and blood vessels; their circulation in the blood and lymph; adhesion to vascular endothelium; re-invasion into surrounding tissues; movement (movement) in tissues; interaction with microenvironment cells; proliferation and formation of a daughter tumor (secondary focus - metastasis).
Angiogenesis in a tumor. The growth of the primary tumor occurs in parallel with the development of small blood vessels (mainly capillaries). The tumor grows into vessels as a result of migration and proliferation of endotheliocytes under the influence of factors that stimulate angiogenesis. These factors are produced both by the tumor itself and by macrophages richly represented in the tumor growth zone. To the most active factors angiogenesis include macrophage fibroblast growth factor, α- and β-transforming growth factors (TGF), platelet-derived growth factor (PGFr), vascular endothelial growth factor (EGF), etc.
Invasion tumor cells into the surrounding tissues, interstitial space and blood vessels includes the following steps:
Separation of individual tumor cells from the primary tumor focus occurs as a result of a weakening of the adhesion (bonds, contacts) between individual tumor cells. Great importance this mechanism has a decrease in the expression of cadherin proteins;
Interaction of detached tumor cells with fibronectin, laminin, extracellular matrix collagen with the help of receptors for these substances formed on tumor cells;
Enzymatic destruction of the extracellular matrix by collagenase, cathepsin D and other proteases produced both by the tumor itself and by stimulated macrophages;
The movement of the tumor cell is provided by the formation of pseudopodia and the contractile activity of actomyosin filaments. Cells move in the direction of action of chemoattractants produced both by surrounding tissues and by the tumor itself.
Circulation of a tumor cell in the blood. In the process of transport, these cells actively interact with platelets, leukocytes, endotheliocytes, and various PAS. Most of the tumor cells are damaged immune system organism, another (smaller) part of them remains viable (resistant) due to protection from immune damage due, first of all, to the formation of platelet aggregates and fibrin clots around them. This is facilitated by the activation of the hemostasis system by enzymes released from tumor cells. Platelet aggregates and fibrin clots with a tumor cell in the center in the form of microemboli can clog small blood vessels and disrupt microcirculation in a particular region of the vascular bed.
Adhesion of tumor cells to vascular endothelium occurs due to embolization of microvessels in the composition of platelet aggregates and fibrin clots. The tumor cell secretes a plasminogen activator, which leads to the activation of fibrinolysis. In this case, the clot lyses, and the released tumor cell adheres to the endothelium.
Repeated invasion of tumor cells into the surrounding tissues at the site of their adhesion occurs according to the same mechanisms as in the primary tumor focus.
The movement of their vessels into the tissues of tumor cells is carried out in the direction of chemoattractants, which can be produced by the tumor cell itself (autochemotaxis).
After the interaction of the tumor cell with the cells of the microenvironment it proliferates and forms a secondary tumor focus , which, depending on the location and type of tumor cells, has a local and general damaging effect on the body of varying intensity.
It has been shown that some malignant tumors can metastasize to various bodies, others - mainly in certain organs (in particular, breast adenocarcinoma more often metastasizes to bones and the brain; stomach cancer - to the liver, etc.).
Recurrence(from lat. recidivus - returning, resuming) - re-development a tumor that usually occurs after incomplete removal of the tumor or as a result of implantation of both tumor cells and oncogenes in surrounding normal tissues.
cachexia(kachexia, from the Greek kacos - bad and hexis - condition) or general atrophy - a syndrome of body exhaustion, characterized by pronounced general emaciation, physical weakness, a decrease in the functioning of life-supporting regulatory (nervous, endocrine, immune, humoral, genetic), executive (cardiovascular, hematopoietic, digestive, etc.) and metabolic (decreased RNA synthesis, tumor necrosis factor, catalase, etc.) systems. A progressively increasing drop in body weight occurs mainly due to the depletion of muscle tissue and fat depots.
Introduction to oncopathology Principles of classification of tumors. Morphological characteristics of benign and malignant tumors from epithelial and mesenchymal tissues Principles of classification of tumors. Morphological characteristics of benign and malignant tumors from epithelial and mesenchymal tissues
Nomenclature and classifications In most names of tumors, the name of an organ or tissue appears as the root of the word, to which the suffix "oma" is added. Examples: hepatoma, meningioma, neurinoma, lipoma fibroma, etc. But there are exceptions regarding malignant neoplasms: carcinoma is a malignant tumor from epithelial tissue, sarcoma is a malignant tumor from non-epithelial tissue. In most names of tumors, the name of an organ or tissue appears as the root of the word, to which the suffix "oma" is added. Examples: hepatoma, meningioma, neurinoma, lipoma fibroma, etc. But there are exceptions regarding malignant neoplasms: carcinoma is a malignant tumor from epithelial tissue, sarcoma is a malignant tumor from non-epithelial tissue.



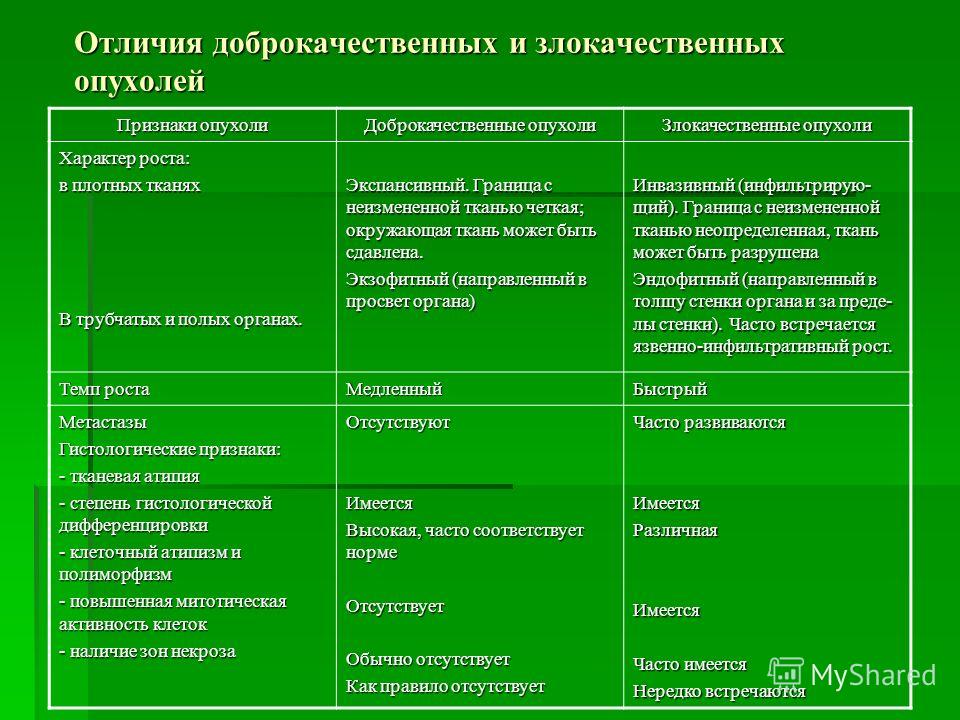
Differences between benign and malignant tumors Signs of a tumor Benign tumors Malignant tumors Character of growth: in dense tissues in tubular and hollow organs. Expansive. The border with unchanged tissue is clear; surrounding tissue may be compressed. Exophytic (directed into the lumen of the organ) Invasive (infiltrating). The border with unchanged tissue is indefinite, the tissue can be destroyed Endophytic (directed into the thickness of the organ wall and beyond the wall). Often there is ulcerative infiltrative growth. Growth rate Slow Rapid Metastases Histological features: - tissue atypia - degree of histological differentiation - cellular atypism and polymorphism - increased mitotic activity of cells - presence of areas of necrosis Absent High, often normal Absent Usually absent As a rule absent Frequently developed





Organ-specific tumors (both benign and malignant) are characterized by the fact that they develop from the epithelial cells of a particular organ and retain the morphological and sometimes functional features of this organ (the production of hormones and biologically active substances by the tumor tissue)
These tumors will be studied in detail in a private course of pathological anatomy. Let's consider just a few of them.
Breast. Tumors are very diverse and often develop against the background of the nodular form of fibrocystic disease.
Fibroadenoma. A benign tumor of the glandular epithelium with a highly developed stroma. It occurs at any age, but more often in 20-45 years. Depending on the diameter of the glandular tubes forming the tumor and the nature of the location of the connective tissue, pericanalicular and intracanalicular fibroadenomas are distinguished. Intracanalicular fibroadenoma is characterized by elongation of the glandular tubes, invagination into their lumen of areas of myxomatous connective tissue, as a result of which the lumen of the duct becomes slit-like. With the concentric growth of the intralobular connective tissue around the ducts, which remain small in size, there is pericanalicular fibroadenoma. Rarely, a leaf-shaped (phylloidal) tumor occurs in which there is a pronounced proliferation of the stromal component.
Mammary cancer. It is the most common neoplasia in women essential role female sex hormones (estrogens) play in its development. Breast cancer is represented by the following main forms: non-infiltrating lobular and ductal cancer, infiltrative forms of these cancers, nipple cancer (Paget's cancer). In addition, there are rare forms of breast cancer, such as mucous cancer, apocrine, etc.
Non-infiltrating (non-invasive) lobular carcinoma. As a rule, it is detected by microscopic examination of the mammary gland, removed for a benign neoplasm. Microscopically built from atypical cells, grows in a lobule, has glandular or solid variants.
Non-infiltrating (non-invasive) ductal carcinoma. Macroscopically, it is represented by dilated ducts, from which crumbling yellowish masses are squeezed out on cuts. Microscopically it can be papillary, cribriform and acneiform (solid proliferates of tumor cells with massive necrosis in the center). Grows within the duct, microcalcifications are often found.
Invasive forms of ductal and lobular cancer are macroscopically represented mainly by dense whitish stellate nodes with yellowish specks. Under microscopy, they consist of scirrhous, cribrous, alveolar and tubular glandular structures with cellular polymorphism.
Paget's cancer. It develops from the epidermis or epithelial cells of large ducts. Large light cells (Paget cells) are formed in the basal and middle layers of the epidermis. The tumor is localized in the area of the nipple and areola.
Currently, along with routine histopathological examination, immunomorphological and molecular biological methods are widely used to predict the course of the disease and a possible response to therapy. Approximately 70% of all breast cancers are positive for estrogen receptor (ER) and/or progesterone (PR) expression. Tumors expressing ER and PR are amenable to hormone therapy. The prognosis of the disease is established as a result of the study of ER, PR, transmembrane receptor for growth factors HER-2 / neu and nuclear protein Ki-67. HER-2-positive cases of breast cancer are characterized by low efficiency of not only hormonal, but also chemotherapy, lower survival rate and flow. Protein Ki-67 is a marker of cell proliferation. The higher the proliferative activity of tumor cells, the worse the prognosis.
Tumors of the endocrine glands.
Adrenals. Tumors arise from the cortical and medulla layers. They can be benign and malignant.
Benign tumors of the cortical layer: Clear cell adrenocortical adenoma (produces aldosterone), dark cell adrenocortical adenoma ( produces androgens, less often - glucocorticosteroids, therefore, there are signs of virilism, less often Cushing's syndrome), mixed adrenocortical adenoma (manifested by hypercorticism - Cushing's syndrome), glomerulocellular adenoma (increased production of mineralocorticoids).
Malignant tumor of the adrenal cortex. adrenocortical cancer : built from atypical polymorphic cells, characterized by predominantly hematogenous metastasis.
Benign brain tumor. Pheochromocytoma: A hormonally active tumor that secretes large amounts of catecholamines (adrenaline and norepinephrine), resulting in high blood pressure (usually malignant hypertension, with severe crises).
Malignant tumor of the adrenal medulla. Malignant pheochromocytoma (pheochromoblastoma): characterized by marked cellular atypism, usually hormonally inactive.
kidneys
Benign tumors - adenomas . Renal adenoma is usually an incidental finding in the study of surgical or autopsy material. Tumor nodes can be single or multiple, located in the cortex of the kidney, reaching a diameter of 10 cm or more. According to the histological structure, they can be acinar, papillary, tubular and solid, cystic. According to the color of the cytoplasm, dark-celled, clear-celled, and acidophilic are distinguished. Clear cell adenoma is built from light polygonal cells with vacuolated cytoplasm containing a large amount of lipids and glycogen. Differential diagnosis of this variant of the tumor with clear cell carcinoma kidneys is exceptionally difficult. It was proposed that a clear cell tumor up to 3 cm in diameter be conventionally attributed to an adenoma, and larger to a cancer. However, this criterion is not reliable enough, since there are known cases of metastases of a clear cell tumor of the kidney with a diameter of 2 cm or even less. In cases of detection of clear cell cancer in another organ in a patient who has undergone nephrectomy for a kidney tumor for a long time, it must be borne in mind that metastases of clear cell cancer can sometimes be observed 5-10 or more years after the operation.
Neuroendocrine tumors (apudomas) develop from apudocyte precursor cells located in almost all organs and having a common origin with the epithelial cells of this organ. Normally, apudocytes carry out local neuroendocrine regulation of organs and are conditionally combined into a diffuse APUD system (diffuse endocrine system). The cells of this system produce many biogenic amines and polypeptide hormones (serotonin, calcitonin, ACTH, growth hormone, intestinal hormones, etc.).
Previously, it was believed that apudoma could be benign and called them carcinoids (malignant variants - atypical carcinoids). But at present, all carcinoids are commonly regarded as potentially malignant tumors (neuroendocrine cancer). Most often, carcinoids (neuroendocrine cancers) develop in the appendix, stomach, and lung. Many adenocarcinomas (lung, endometrium, colon, etc.) may contain tumor cells with neuroendocrine differentiation.
Neuroendocrine cancers and other tumors with neuroendocrine cells are the cause of the development of ectopic endocrine syndromes (Cushing, Zollinger-Ellison, Kohn, acromegaly, etc.).
Leather
Benign tumors of the sweat glands - papillary hydradenoma, eccrine spiradenoma, syringoma, etc. Malignant analogue- cancer of the sweat glands.
Basal cell carcinoma (obsolete - basalioma) is the most common malignant tumor of the skin. It belongs to the group of tumors with locally destructive growth, often recurs, but never gives metastases (the available descriptions of metastases are doubtful). It is localized more often on the face, neck, it is multiple, often ulcerated. Macroscopically, it is a plaque, nodule, or deep ulcer. Microscopically characteristic are polymorphic strands and complexes of small intensely stained cells (similar to basal cells of stratified squamous epithelium), which have a prismatic shape along the periphery of the strand, and a polygonal shape in its thickness. Mitoses are rare.