Gynecological examinations during pregnancy in the antenatal clinic. Examinations during pregnancy
I The trimester of pregnancy is decisive in predicting its outcome for the mother and fetus, so an in-depth examination of the woman's health status and identification of prenatal risk factors is necessary.
The first examination is carried out at 8-14 weeks of pregnancy. Further, the schedule of mandatory examinations includes the terms of gestation: 20-24 weeks, 36-38 weeks, 40-41 weeks.
The main tasks of the survey in I trimester the following:
Establishing the presence of pregnancy, determining its duration, the date of the expected birth. If necessary, the question of the duration of pregnancy is decided taking into account the ultrasound data.
Examination of the health status of a pregnant woman to identify risk factors for the development of maternal and fetal complications. After the first examination by an obstetrician-gynecologist, the pregnant woman is sent for examination to a therapist who examines her twice during pregnancy (in the early stages and at 30 weeks of pregnancy). The pregnant woman is also consulted by other specialists (dentist, ophthalmologist, otorhinolaryngologist and, if indicated, by other specialists).
Deciding on the possibility of maintaining or recommending termination of pregnancy if it threatens life or poses a danger of the birth of a sick handicapped child.
Drawing up an individual examination plan and conducting an algorithm for prenatal monitoring.
Prevention and treatment of complications during pregnancy.
At the first communication between a doctor and a pregnant woman, the following is necessary:
1. Reveal:
Features of the anamnesis (family, gynecological, obstetric). When reviewing a family history, one should highlight the presence of diabetes mellitus, hypertension, tuberculosis, mental and oncological diseases, multiple pregnancies in relatives, the presence of children with congenital and hereditary diseases in the family. The obstetric and gynecological history includes information about the characteristics of the menstrual cycle, the number of pregnancies, the intervals between them, the outcomes of childbirth, the weight of newborns, the development and health of children. We also need data on abortions and their complications, surgeries, gynecological diseases, and infertility. It is important to identify whether there were any laparoscopic operations, including the removal of myomatous nodes.
Past and concomitant diseases, medications taken, the presence of allergies. It is necessary to obtain information about such past diseases as rubella, toxoplasmosis, genital herpes, cytomegalovirus infection, chronic tonsillitis, diseases of the kidneys, lungs, liver, cardiovascular, endocrine systems, oncological pathology, increased bleeding, operations, blood transfusion, allergic reactions.
The nature of work, lifestyle, bad habits, occupational hazards.
2. Conduct a general clinical and special (gynecological and obstetric) examination.
At the first examination of a pregnant woman, height, body type, body weight, and pelvic dimensions are assessed. They measure blood pressure on both hands, examine the condition of the heart, respiratory organs, thyroid and mammary glands, liver, and abdominal organs. A vaginal examination is mandatory (examination of the cervix and vagina with the help of mirrors, the size of the uterus, its consistency, tone, the area of \u200b\u200bthe appendages).
At 10 weeks of gestation, blood pressure should be recorded. With the normal development of pregnancy, it should be in the range of 120/80-115/70 mm Hg. Art. The presence of hypertension during this period is the basis for an in-depth examination for renal pathology or the presence of hypertension, as well as the possibility of reduced production of PGE 2 (primary placental insufficiency). It is important at this time to identify the peak of CG secretion, confirming the function of the trophoblast.
3. Research: blood tests with the definition of the group, Rh affiliation, coagulogram, hematocrit, acetone level, ketone bodies (according to indications); as well as blood tests for HIV, RW , Hbs , HCV . A general urine test allows you to roughly judge the condition of the kidneys.
4. Conduct a study on the most common infections, which are leading in the formation of complications of pregnancy and the occurrence of congenital malformations. This group TORCH - infections (toxoplasmosis, rubella, cytomegalovirus, herpes, etc.). If antibodies to the rubella virus, CMV, toxoplasma are not detected, the patient is at risk for primary infection during pregnancy, which is especially dangerous for the fetus.
Based on the data obtained, there may be grounds for testing for diabetes, tuberculosis, syphilis, etc.
It is necessary to conduct bacteriological and virological examination of the vaginal contents. It is necessary to investigate not the translucent, but the parietal flora (scraping of the mucous membrane).
A screening ultrasound scan should be performed to clarify the gestational age, assess the size of the ovum, embryo, fetus, determine the number of embryos, as well as the length of the cervix and the size of the internal os if a threatened miscarriage is suspected.
Primary laboratory studies:
1. Clinical blood test.
2. General analysis of urine.
3. Coagulogram, antibodies to hCG, antibodies to lupus antigen.
4. Determination of glucose content in the blood.
5. Blood type, Rh -factor, determination of anti-Rhesus antibodies.
6. Serodiagnosis of syphilis, HIV infection, hepatitis.
7. Determination of antibody titer to rubella virus, toxoplasmosis.
8. Determination of the level of 17-KS (according to indications).
9. Examination for urogenital infection.
Determination of hemoglobin and hematocrit. According to WHO definition, anemia of pregnant women is considered to be a decrease in hemoglobin levels below 100 g / l, hematocrit - below 30%. In such cases, it is necessary to examine the pregnant woman to determine the cause of the disease.
The study of the middle portion of urine for the presence of protein, glucose, bacteria, leukocytes. If a pregnant woman has kidney disease, it is necessary to determine the prognosis of pregnancy for the mother and fetus, prevent the occurrence of possible complications during the development of pregnancy, prescribe appropriate therapy and, if necessary, hospitalize in a specialized hospital.
Coagulogram and determination of antibodies. The risk group for the presence of autoantibodies to phospholipids is the following category of women with a history of:
Habitual miscarriage of unknown origin;
intrauterine fetal death II and III trimesters of pregnancy;
Arterial and venous thromboses, cerebrovascular diseases;
Thrombocytopenia of unknown origin;
False positive reactions to syphilis;
Early toxicosis, preeclampsia;
Retardation of intrauterine development of the fetus;
Autoimmune diseases.
In the presence of antiphospholipid antibodies in I trimester of pregnancy is determined by hyperfunction of platelets. The degree of hypercoagulability of the plasma link of hemostasis increases. As a result of hyperfunction of platelets and hypercoagulation of the plasma link of hemostasis, thrombosis and heart attacks occur in the placenta, markers of activation of intravascular coagulation - PDF and soluble complexes of fibrin monomers are determined. All these disorders can lead to thrombosis of the vessels of the placenta and death of the fetus.
It is necessary to emphasize the particular importance of early initiation of therapy in patients with APS due to the damaging effect of lupus antigens on the vessels of the placental site. The detected disorders of the hemostasis system are an indication for the use of antiplatelet agents and anticoagulants against the background of glucocorticosteroid therapy. For the relief of hemostatic disorders, it is prescribed from 9-10 weeks of pregnancy and later:
Prednisolone or metipred 2.5-5 mg / day;
Curantil 75.0 mg/day one hour before meals;
Trental 300.0 mg/day;
Fraxiparine 0.3 ml 2 times subcutaneously or small doses of heparin from 10,000 to 30,000 IU / day (the duration of heparin therapy is determined by the severity of hemostasiological disorders).
This treatment regimen is optimal for gestation periods up to 20 weeks and can be used repeatedly until delivery.
Control of the hemostasis system is carried out 1 time in 2 weeks.
With autosensitization to hCG or pregnancy proteins associated with hCG, hemostasis disorders in I trimester are also expressed, which is an indication for heparin therapy.
Determination of glucose content in the blood. All pregnant women undergo a scanning study to detect diabetes by determining the concentration of glucose on an empty stomach and 1 hour after taking 50 g of glucose. If the fasting blood glucose level is above 5.00 mmol / l, one hour after taking 50 g of glucose - more than 7.77 mmol / l, as well as in the presence of risk factors (glucosuria, a family history of aggravated diabetes), a test for glucose tolerance.
Determination of the blood group, Rh -factor and anti-Rhesus antibodies. All pregnant women should undergo a blood test in order to timely identify Rh -isoimmunization, which is especially often the cause of the most severe forms of fetal hemolytic disease. Other isoantibodies can also cause serious complications.
Serodiagnosis of syphilis, HIV infection, hepatitis. Seropositive women may be advised to terminate the pregnancy. The risk of vertical transmission of infection is at least 24%. The fetus becomes infected with syphilis II trimester.
Hepatitis B screening results may indicate that a newborn needs immunoglobulin and hepatitis B vaccine immediately after birth. The risk of transmission early in pregnancy is low.
Determination of antibodies to rubella virus and toxoplasmosis. Positive rubella serological test results due to primary infection during I trimester of pregnancy indicate a high risk of congenital anomalies, so it is advisable to recommend termination of pregnancy.
Rubella screening appears to be useful because negative tests can alert the patient that contact with an infected person is dangerous for her infant and suggest active immunization after delivery.
If a pregnant woman is diagnosed with acute toxoplasmosis, there may be a question of terminating the pregnancy for medical reasons. It should be noted that most of these women give birth to an infected child.
Determination of the level of 17-KS in daily urine, the level of GDEA to determine the source of hyperandrogenism. 17-CS is determined every 2-3 weeks to adjust the dose of dexamethasone. Monitoring the course of pregnancy in women with hyperandrogenism should be carried out taking into account the critical periods of pregnancy characteristic of this pathology: 13 weeks (release of testosterone by the ovaries of the male fetus), 20-24 weeks (the beginning of hormonal production of the adrenal cortex), 28 weeks (release of ACTH by the pituitary gland fetus).
In addition to dexamethasone, with the threat of termination of pregnancy in I trimester, it is advisable to use hCG at 1500 IU intramuscularly once a week. With combined and ovarian hyperandrogenism, severe hyperestrogenism, it is advisable to prescribe natural (but not synthetic) gestagen preparations. With adrenal hyperandrogenism, the appointment of gestagens is not justified, since in most cases there is an increased content of progesterone.
Examination for urogenital infection. Given the widespread prevalence of urogenital infection among the population in terms of preconception preparation and during pregnancy, it is necessary to conduct a laboratory examination for the presence of a sexually transmitted infection:
Examination of scrapings from the cervical canal and urethra by the method PCR for the presence of bacteriaChlamydia, Mycoplasma, Ureaplasma, family virusesherpesviridae - BUT and CMV;
Determination in blood serum by ELISA of antibodies of class M and G to C. Trachomatis, M. Hominis, HSV-1, HSV-2, CMV;
Microscopic examination of vaginal, cervical and urethral discharge.
Pregnant women with urogenital infection should be identified as a high-risk group for the possibility of having a child with intrauterine infection, morphofunctional immaturity and malnutrition.
echographic scan. Sonography is the most important tool for examining a pregnant woman and can be used according to clinical indications at any stage of pregnancy.
In early pregnancy, ultrasound is performed for:
Confirmation of pregnancy;
Clarification of the gestational age;
Clarification of the location of the fetal egg;
Detection of multiple pregnancy;
Exceptions of hydatidiform mole;
Exclusion of formations in the small pelvis or hormonally active ovarian tumors;
Diagnosis of uterine fibroids or ovarian formations that could interfere with the normal course of childbirth.
Ultrasound can detect:
Hypoplasia of the embryo;
Non-immune dropsy;
Cystic hygroma of the neck;
anencephaly;
spina bifida;
Cephalocele;
Choroid plexus cysts of the lateral ventricles of the brain;
Splitting of the hard palate;
polydactyly;
Diaphragmatic hernia;
sacrococcygeal teratomas;
agenesis of the kidneys;
Polycystic kidney disease;
Consolidated twins.
Ultrasound diagnostics are available:
Most of the defects of the limbs;
Hydronephrosis;
Polycystic kidney disease;
Gastroschisis (splitting of the anterior abdominal wall of the fetus);
Facial clefts;
Defects of the nervous system.
Generally accepted indications for medical genetic counseling and in-depth prenatal examination:
1. Late age of parents (mothers aged 35 and over).
2. The presence in the anamnesis of a child with intrauterine malformations.
3. Hereditary diseases in the family.
4. Consanguineous marriage.
5. Occupational hazards (chemical production, radiation exposure and UVI).
6. Bad habits (alcohol, drugs).
7. Taking teratogenic drugs (antidepressants, tetracycline, codeine, antithyroid drugs, etc.).
8. Acute viral diseases during pregnancy.
9. The threat of termination of pregnancy from an early date.
10. Spontaneous miscarriages in history.
Invasive diagnostics. Indications for invasive methods of prenatal diagnosis in Itrimester (chorionic biopsy, amniocentesis, cordocentesis, placentocentesis):
The age of the pregnant woman is over 35;
Chromosomal aberrations in one of the spouses;
A history of a child with intrauterine malformations or chromosomal abnormalities;
The presence of congenital malformations or echomarkers of fetal developmental disorders;
Change in the level of AFP and HCG;
X-linked diseases in the family.
Invasive interventions are carried out with the consent of the pregnant woman under ultrasound control by a trained medical specialist in order to obtain fetal cells and determine the genetic state of the fetus based on them.
When terminating a pregnancy within 12 weeks, direct methods of genetic diagnosis are used, which are used during the prenatal examination of a pregnant woman.
A selected sample of fetal tissue after termination of pregnancy should be identified on the basis of cytomorphological examination.
Additional research methods (according to indications):
Hormonal;
Biochemical;
Immunological;
Hematological:
lupus anticoagulant,
API;
Invasive methods of prenatal diagnosis (amniocentesis, chorionic biopsy).
The volume of examination of pregnant women is presented in Table. 1 .
Table 1 . Standard for clinical and laboratory examination of pregnant women in I trimester Initial treatment (up to 12 weeks)
Physical examination: measurement of body weight, height, blood pressure (on both arms), palpation of the thyroid gland, mammary glands, auscultation of the heart and lungs, examination of the abdomen and extremities, examination by a dentist Gynecological examination: bimanual vaginal examination, cytological analysis of vaginal discharge and smears from cervical canal (diagnosis of chlamydia), determination of the configuration and size of the uterus and the condition of the appendages, external pelvimetry, examination of the cervix in the mirrors
Poll. The first meeting with a pregnant woman, as a rule, takes place in outpatient settings (antenatal clinic, perinatal centers), but it also happens in a hospital. At the first visit of the patient, the doctor should conduct a survey with a thorough history taking (general and obstetric-gynecological), assess the general condition, genital organs and, if necessary, use additional examination methods. All the information received is recorded in the outpatient card of the pregnant woman or in the history of childbirth in the hospital.
Passport data. Pay attention to the age of the pregnant woman, especially the primipara. The complicated course of pregnancy and childbirth is more often observed in "elderly" (over 30 years old) and "young" (under 18 years old) primiparas. The age of a pregnant woman 35 years and older requires prenatal diagnosis due to a higher risk of having a child with congenital and hereditary pathologies.
Complaints. First of all, they find out the reasons that prompted the woman to seek medical help. A visit to the doctor in the first trimester of pregnancy is usually associated with the cessation of menstruation and the assumption of pregnancy. Often during this period of pregnancy, patients complain of nausea, vomiting and other health disorders. With a complicated course of pregnancy (a miscarriage that has begun, an ectopic pregnancy, concomitant gynecological diseases), there may be bloody discharge from the genital tract. Complaints about violations of the functions of internal organs may be due to extragenital diseases (cardiovascular, diseases of the respiratory system, kidneys, digestive system, etc.).
The complaints of pregnant women should be treated very carefully and recorded in a medical document.
Working and living conditions. Professional, domestic and environmental hazards that can adversely affect the course of pregnancy and fetal development are carefully ascertained (living in environmentally unfavorable regions, hard physical labor, work associated with vibration, chemicals, a computer, prolonged static loads, etc.). Be sure to ask questions about smoking (including passive), alcoholism, drug addiction.
Heredity and past diseases. They find out if the family of the pregnant woman and / or her husband had multiple pregnancies, hereditary diseases (mental diseases, blood diseases, metabolic disorders), as well as congenital and hereditary developmental anomalies in the next of kin.
It is necessary to obtain information about all previously transferred diseases, starting from childhood. So, for example, rickets suffered in childhood can cause pelvic deformity, which will complicate the course of rolls. Indirect signs of transferred rickets are late teething and the beginning of walking, skeletal deformities, etc. Poliomyelitis, tuberculosis in childhood can also lead to violations of the pelvic structure. Measles, rubella, rheumatism, tonsillitis, recurrent tonsillitis and other infectious diseases often cause girls to lag behind in physical and sexual development. Diphtheria of the vulva and vagina may be accompanied by the formation of cicatricial constrictions.
Non-communicable and infectious diseases transferred in adulthood are also clarified. Diseases of the cardiovascular system, liver, lungs, kidneys and other organs can complicate the course of pregnancy and childbirth, and pregnancy and childbirth can, in turn, exacerbate chronic diseases or cause relapses.
If there was a history of surgical interventions, then it is better to obtain medical documents about them with recommendations from specialists on the tactics of conducting a real pregnancy and childbirth. Of great importance are information about past injuries (skull, pelvis, spine, etc.).
menstrual function. Find out at what age the first menstruation appeared (menarche), after what period of time regular menstruation was established; the duration of the menstrual cycle, the duration of menstruation, the amount of blood lost, soreness; whether the nature of menstruation has changed after the onset of sexual activity, childbirth, abortion; first day of last menstruation.
sexual function. They collect information about the onset of sexual activity, find out what marriage is in a row, whether there are pains and bloody discharge during sexual intercourse, what methods of contraception were used before pregnancy, and the interval from the beginning of regular sexual activity to the onset of pregnancy. The absence of pregnancy within 1 year of regular sexual activity without the use of contraceptives may indicate infertility and indicate certain disorders of the reproductive system.
Information about the husband (partner) of the pregnant woman is also required: his state of health, age, profession, smoking, alcoholism, drug addiction.
Gynecological history. It is necessary to obtain information about past gynecological diseases that may affect the course of pregnancy, childbirth and the postpartum period (uterine fibroids, tumors and tumor-like formations of the ovaries, diseases of the cervix, etc.). Particular attention should be paid to previous surgical interventions on the genitals, primarily on the uterus, leading to the formation of a scar (myomectomy). An extract from a medical institution with a detailed description of the operation performed is required. For example, in case of myomectomy, it is necessary to obtain information about the access of surgical intervention (laparotomic or laparoscopic), with or without opening the uterine cavity, etc.
Find out the pregnant woman's complaints about pathological discharge from the genital tract (abundant, purulent, mucous, bloody, etc.), which may indicate a gynecological disease.
It is important to get information about past sexually transmitted diseases (HIV infection, syphilis, gonorrhea, chlamydia, etc.).
Obstetric history. First of all, it is necessary to clarify what the real pregnancy is (first, repeated) and what kind of childbirth is coming.
In foreign literature, the following concepts are distinguished.
- Nulligravida - a woman who is not currently pregnant and has no history of pregnancy.
- Gravida - a woman who is currently pregnant or has had pregnancies in the past, regardless of their outcome. During the first pregnancy, a woman is considered primigravida (primigravida), and in subsequent pregnancies - re-pregnant (multigravida).
- Nullipara - a woman who has never had a pregnancy that has reached the term of a viable fetus; she may or may not have previously had pregnancies that ended in abortion at an earlier date.
- Primipara - a woman who carried one pregnancy (single or multiple) to the term of the birth of a viable fetus.
- Multipara - a woman with a history of several pregnancies, full-term to the term of a viable fetus (22 weeks of pregnancy, fetal weight 500 g, height 32-34 cm).
Note the number of artificial or spontaneous abortions (miscarriages). If there were abortions, then at what stage of pregnancy, were they accompanied by complications (endometritis, inflammatory diseases of the uterus, perforation of the uterus, etc.). If possible, specify the cause of spontaneous abortion. Abortions preceding pregnancy can lead to miscarriage, a pathological course of childbirth.
Multiparous women receive detailed information about how previous pregnancies and childbirth proceeded. If there were complications of pregnancy (preeclampsia, miscarriage, etc.), then detailed information is needed about this, since they are important in predicting the course and outcome of this pregnancy and the upcoming birth. Find out whether the birth was timely, premature or late, spontaneous or operative (caesarean section, obstetric forceps, vacuum extraction of the fetus).
When delivering by caesarean section, it is necessary to clarify, if possible, the indications for it, whether it was performed on a planned or emergency basis, how the postoperative period proceeded, on what day after the operation the patient was discharged.
When taking an obstetric history, special attention should be paid to the condition of the child at birth (weight, length, Apgar score, whether the child was discharged from the maternity hospital or transferred to the 2nd stage of nursing and in connection with this), as well as the psychophysical development of the child at present day. In case of an unfavorable outcome, it is necessary to find out at what stage the death of the fetus / newborn occurred: during pregnancy (antenatal death), during childbirth (intranatal death), in the early neonatal period (postnatal death). It should also clarify the possible cause of death (asphyxia, birth trauma, hemolytic disease, malformations, etc.).
Detailed information about the course and outcomes of previous pregnancies and childbirth allows us to identify high-risk patients who need special attention and more careful monitoring.
Objective examination. After getting acquainted with the anamnesis, the patients proceed to an objective study, which begins with an examination.
At examination pay attention to the growth of the pregnant woman, physique, fatness, the condition of the skin, visible mucous membranes, mammary glands, the size and shape of the abdomen.
The skin during pregnancy may have certain features: pigmentation of the face, nipple area, white line of the abdomen. In the second half of pregnancy, so-called pregnancy bands often appear. Combs, ulcers on the skin require a special examination. Paleness of the skin and visible mucous membranes, cyanosis of the lips, yellowness of the skin and sclera, swelling are signs of a number of serious diseases.
The objective signs of a former pregnancy and childbirth include a decrease in the tone of the muscles of the anterior abdominal wall, the presence of striae gravidarum.
Pay attention to the physique, possible deformations of the skeleton, as they can affect the structure of the pelvis.
Violations of the hormonal regulation of the reproductive system can lead to underdevelopment of the mammary glands, insufficient expression of hair growth in the axillary region and on the pubis, or, conversely, excessive hair growth on the face, lower extremities, and along the midline of the abdomen. In women, the features of masculinization are possible - broad shoulders, male structure of the pelvis.
The severity of subcutaneous adipose tissue should be assessed. Both alimentary and endocrine obesity of the II-III degree adversely affects the course of pregnancy and childbirth.
Measure the height and determine the body weight of the pregnant woman. When determining body weight, one should take into account not its absolute values, but the body mass index, which is calculated taking into account the height of the patient [body weight in kilograms / (height in meters) 2], which is normally 18-25 kg / m2. With low stature (150 cm and below), narrowing of the pelvis of varying degrees is often observed, women of high stature often have a male-type pelvis.
Examination of the abdomen in the third trimester of pregnancy allows you to find out deviations from its normal course. In normal pregnancy and the correct position of the fetus, the abdomen has an ovoid (ovoid) shape; with polyhydramnios, the abdomen is spherical, its size exceeds the norm for the expected gestational age; in the transverse position of the fetus, the abdomen takes the form of a transverse oval. With overstretching or divergence of the muscles of the anterior abdominal wall (more often in multiparous), the abdomen may be sagging. The shape of the abdomen also changes with a narrow pelvis.
Examination of internal organs(cardiovascular system, lungs, digestive organs, kidneys), as well as the nervous system, is carried out according to the system generally accepted in therapy.
Obstetric examination includes determining the size of the uterus, examining the pelvis, assessing the position of the fetus in the uterus based on special obstetric techniques. Methods of obstetric examination depend on the gestational age.
In the first trimester of pregnancy, the size of the uterus is determined by a two-handed vaginal-abdominal examination, which begins with an examination of the external genital organs. The study is carried out in sterile rubber gloves on a gynecological chair. The woman lies on her back, her legs are bent at the hip and knee joints and divorced; when examining on a bed, a roller is placed under the sacrum.
The external genital organs are treated with an antiseptic solution. The large and small labia are parted with I and II fingers of the left hand and examine the external genital organs (vulva), the mucous membrane of the entrance to the vagina, the external opening of the urethra, the excretory ducts of the large glands of the vestibule and the perineum.
In order to examine the walls of the vagina and cervix, examination with mirrors. This determines the cyanosis due to pregnancy, and various pathological changes in the disease of the vagina and cervix. Vaginal mirrors (Fig. 6.1) are folding, spoon-shaped, metal or plastic. The folded speculum is inserted to the fornix of the vagina in a closed form, then the folds are opened, and the cervix becomes available for inspection. The walls of the vagina are examined with the gradual removal of the mirror from the vagina.
Rice. 6.1. Vaginal mirrors (A - folding, B - spoon-shaped, C - lift)With a vaginal (finger) examination fingers of the left hand spread large and small labia; the fingers of the right hand (II and III) are inserted into the vagina, the I finger is retracted upward, IV and V are pressed against the palm and rest against the perineum. This determines the condition of the muscles of the pelvic floor, the walls of the vagina (folding, extensibility, loosening), the vaults of the vagina, the cervix (length, shape, consistency) and the external pharynx of the cervix (closed, open, round or slit-like).
An important criterion for former births is the shape of the external os of the cervix, which in those who have given birth has the shape of a longitudinal slit, and in those who have not given birth it is round or punctate (Fig. 6.2). Women who have given birth may have cicatricial changes after ruptures of the cervix, vagina and perineum.

After palpation of the cervix, proceed to two-handed vaginal-abdominal examination(Fig. 6.3). With the fingers of the left hand, gently press on the abdominal wall towards the pelvic cavity towards the fingers of the right hand, located in the anterior fornix of the vagina. Bringing together the fingers of both examining hands, palpate the body of the uterus and determine its position, shape, size and consistency. After that, they begin to study the fallopian tubes and ovaries, gradually moving the fingers of both hands from the corner of the uterus to the side walls of the pelvis. To determine the capacity and shape of the pelvis, the inner surface of the bones of the pelvis, sacral cavity, side walls of the pelvis and symphysis are examined.

When examining a pregnant woman in the II-III trimesters, it is necessary to measure the circumference of the abdomen at the level of the navel (Fig. 6.4) and the height of the fundus of the uterus (Fig. 6.5) with a centimeter tape when the woman is lying on her back. The height of the fundus of the uterus above the pubic joint can also be determined by a tazomer. These measurements are carried out at each visit to the pregnant woman and compare the data obtained with gestational standards.


Normally, by the end of pregnancy, the abdominal circumference does not exceed 100 cm, and the height of the uterine fundus is 35-36 cm. An abdominal circumference of more than 100 cm is usually observed with polyhydramnios, multiple pregnancy, large fetus, transverse position of the fetus and obesity.
Determining the size of the pelvis seems extremely important, since their decrease or increase can lead to a significant disruption in the course of labor. The dimensions of the small pelvis are of the greatest importance during childbirth, which are judged by measuring certain sizes of the large pelvis using a special tool - a tazomer (Fig. 6.6).

The tazomer has the form of a compass, equipped with a scale on which centimeter and half-centimeter divisions are applied. At the ends of the branches of the tazomer there are buttons that are applied to the protruding points of the large pelvis, somewhat squeezing the subcutaneous fatty tissue. To measure the transverse size of the outlet of the pelvis, a tazomer with crossed branches was designed.
The pelvis is measured with the woman lying on her back with her stomach bare and her legs folded. The doctor becomes to the right of the pregnant woman facing her. The branches of the tazomer are picked up in such a way that the I and II fingers hold the buttons. The scale with divisions is directed upwards. Forefingers feel for the points, the distance between which is to be measured, pressing the buttons of the parted branches of the tazomer to them. On the scale mark the value of the corresponding size.
Determine the transverse dimensions of the pelvis - distantia spinarum, distantia cristarun, distantia trochanterica and straight size - conjugata externa.
Distantia spinarum - distance between the anterior superior iliac spines. The buttons of the tazomer are pressed against the outer edges of the anterior superior spines. This size is usually 25-26 cm (Fig. 6.7, a).
Distantia cristarum - the distance between the most distant points of the iliac crests. After measurement distantia spinarum the buttons of the tazomer are moved from the spines but to the outer edge of the iliac crests until the greatest distance is determined. On average, this size is 28-29 cm (Fig. 6.7, b).
Distantia trochanterica - distance between the greater trochanters of the femur. The most protruding points of the large skewers are determined and the buttons of the tazomer are pressed against them. This size is 31-32 cm (Fig. 6.7, c).
The ratio of transverse dimensions is also important. Normally, the difference between them is 3 cm; a difference of less than 3 cm indicates a deviation from the norm in the structure of the pelvis.
Conjugata externa- external conjugate, allowing to indirectly judge the direct size of the small pelvis. To measure it, a woman should lie on her left side, bending her left leg at the hip and knee joints, and keep her right leg extended. The button of one branch of the tazomer is placed in the middle of the upper outer edge of the symphysis, the other end is pressed against the supracacral fossa, which is located under the spinous process of the V lumbar vertebra, corresponding to the upper corner of the sacral rhombus. You can determine this point by sliding your fingers down the spinous processes of the lumbar vertebrae. The fossa is easily identified under the projection of the spinous process of the last lumbar vertebra. The outer conjugate is normally 20-21 cm (Fig. 6.7, d).

The external conjugate is important - by its size one can judge the size of the true conjugate (the direct size of the entrance to the small pelvis). To determine the true conjugate, subtract from the length of the outer conjugate9 cm. For example, if the outer conjugate is20 cm, then the true conjugate is11 cm; if the outer conjugate has a length18 cm, then the true value is equal to9 cmetc.
The difference between the external and true conjugate depends on the thickness of the sacrum, symphysis and soft tissues. The thickness of the bones and soft tissues in women is different, so the difference between the size of the outer and true conjugates does not always correspond exactly to 9 cm. The true conjugate can be more accurately determined by the diagonal conjugate.
Diagonal conjugate ( conjuigata diagonalis) is the distance between the lower edge of the symphysis and the most protruding part of the promontory of the sacrum. This distance can be measured only during vaginal examination, if the middle finger reaches the sacral promontory (Fig. 6.8). If this point cannot be reached, then the distance exceeds 12.5-13 cm and, therefore, the direct size of the entrance to the pelvis is within the normal range: equal to or greater than 11 cm. If the sacral cape is reached, then the point of contact with the lower edge is fixed on the arm symphysis, and then measure this distance in centimeters.

To determine the true conjugate, 1.5–2 cm is subtracted from the size of the diagonal conjugate.
If during the examination of a woman there is a suspicion of a narrowing of the exit of the pelvis, then the dimensions of the exit plane are determined.
The dimensions of the outlet of the pelvis are determined as follows. The woman lies on her back, her legs are bent at the hip and knee joints, divorced and pulled up to the stomach.
Straight size the exit of the pelvis is measured with a conventional tazometer. One button of the tazomer is pressed to the middle of the lower edge of the symphysis, the other to the top of the coccyx (Fig. 6.9, a). The resulting size (11 cm) is larger than the true one. To determine the direct size of the pelvic outlet, subtract 1.5 cm (tissue thickness) from this value. In a normal pelvis, the direct size of the plane is 9.5 cm.
Transverse dimension exit - the distance between the inner surfaces of the ischial bones - is quite difficult to measure. This size is measured with a centimeter or a pelvis with crossed branches in the position of a woman on her back with her legs brought to her stomach. There is subcutaneous fatty tissue in this area, so 1-1.5 cm is added to the resulting size. Normally, the transverse size of the pelvic outlet is 11 cm (Fig. 6.9, b).


In the same position, women measure the characteristics of the small pelvis pubic angle, applying I fingers to the pubic arches. With normal size and normal shape of the pelvis, the angle is 90 °.
When deforming the pelvic bones, the oblique dimensions of the pelvis are measured. These include:
The distance from the anterior superior iliac spine of one side to the posterior superior spine of the other side and vice versa;
Distance from the upper edge of the symphysis to the right and left posterior superior spines;
Distance from the supra-sacral fossa to the right or left anterior superior spines.
The oblique dimensions of one side are compared with the corresponding oblique dimensions of the other. With a normal structure of the pelvis, the size of the paired oblique dimensions is the same. A difference greater than 1 cm indicates an asymmetric pelvis.
If necessary, to obtain additional data on the size of the pelvis, its compliance with the size of the fetal head, deformities of the bones and their joints, an X-ray examination of the pelvis is performed - X-ray pelviometry (according to indications).
For the purpose of an objective assessment of the thickness of the pelvic bones, the circumference of the pregnant woman's wrist joint is measured with a centimeter tape (Soloviev's index; Fig. 6.10). The average value of this circumference is 14 cm. If the index is larger, it can be assumed that the pelvic bones are massive and the dimensions of its cavity are smaller than would be expected from the results of measuring the large pelvis.

Indirect signs of the correct physique and normal size of the pelvis are the shape and size of the sacral rhombus (Michaelis rhombus). The upper border of the Michaelis rhombus is the last lumbar vertebra, the lower one is
sacrococcygeal articulation, and the lateral angles correspond to the posterior superior iliac spines (a sacral rhombus of the classical form can be seen at the statue of Venus de Milo). Normally, pits are visible in all four corners (Fig. 6.11). The dimensions of the rhombus are measured with a centimeter tape, normally the longitudinal size is 11 cm, the transverse size is 10 cm.

External obstetric examination. obstetric terminology. The abdomen is palpated in the position of the pregnant woman on her back with her legs bent at the hip and knee joints. The doctor is to the right of the pregnant woman facing her.
On palpation of the abdomen, the condition of the abdominal wall, rectus abdominis muscles is determined (if there are any discrepancies, hernial protrusions, etc.). The tone of the muscles of the abdominal wall is of great importance for the course of childbirth.
Then they proceed to determine the size of the uterus, its functional state (tone, tension during the study, etc.) and the position of the fetus in the uterine cavity.
Of great importance is the determination of the position of the fetus in the uterus. In the III trimester of pregnancy, especially before childbirth and during childbirth, determine the articulation, position, position, appearance, presentation of the fetus (Fig. 6.12).

During palpation of the abdomen, the so-called external methods of obstetric research (Leopold's methods) are used. Leopold (1891) proposed a system of palpation of the abdomen and typical palpation techniques that have received universal recognition.
First external obstetric examination(Fig. 6.13, a). The goal is to determine the height of the uterine fundus and the part of the fetus located in its fundus.
The palms of both hands are placed on the uterus in such a way that they tightly cover its bottom, and the fingers are turned with the nail phalanxes to each other. Most often, at the end of pregnancy, the buttocks are determined in the bottom of the uterus. Usually it is not difficult to distinguish them from the head, since the pelvic end is less dense and does not have a clear sphericity.
The first external obstetric examination makes it possible to judge the gestational age (by the height of the fundus of the uterus), the position of the fetus (if one of its large parts is determined in the fundus of the uterus, then there is a longitudinal position) and presentation (if the buttocks are determined in the fundus of the uterus , then the presenting part is the head).
Second external obstetric examination(Fig. 6.13, b). The goal is to determine the position of the fetus, which is judged by the location of the back and small parts of the fetus (handles, legs).

Hands are shifted from the bottom of the uterus to its right and left sides to the level of the navel and below. Gently pressing the palms and fingers of both hands on the side walls of the uterus, determine which way the back and small parts of the fetus are facing. The backrest is recognized as a wide and curved surface. Small parts of the fetus are determined on the opposite side in the form of small mobile tubercles. In multiparous women, due to the flabbiness of the abdominal wall and the muscles of the uterus, small parts of the fetus are more easily palpated.
By the direction in which the back of the fetus is facing, its position is recognized: the back to the left is the first position, the back to the right is the second position.
In the process of conducting the second appointment of an external obstetric examination, it is possible to determine the excitability of the uterus. Excitability is increased if the uterus tenses in response to palpation. You can determine the increased amount of amniotic fluid by the symptom of fluctuation -
one hand takes the push of the opposite.
The third reception of external obstetric examination(Fig. 6.13, c). Target -
determine the presenting part and its relation to the small pelvis.
One, usually right, hand covers the presenting part, after which they carefully move this hand to the right and left. This technique allows you to determine the presenting part (head or buttocks), the ratio of the presenting part to the entrance to the small pelvis (if it is mobile, then it is located above the entrance to the pelvis, if it is motionless, then it stands at the entrance to the pelvis or in deeper parts of the small pelvis).
The fourth reception of external obstetric examination(Fig. 6.13, d). Target -
determine the presenting part (head or buttocks), the location of the presenting part (above the entrance to the small pelvis, in the entrance or deeper, where exactly), in what position is the presenting head (bent or unbent).
The doctor becomes facing the legs of a pregnant or woman in labor and puts his palms on both sides of the lower part of the uterus. With the fingers of both hands facing the entrance to the pelvis, carefully and slowly penetrate between the presenting part and the lateral sections of the entrance to the pelvis and palpate the available areas of the presenting part.
If the presenting part is movable above the entrance to the pelvis, the fingers of both hands can be brought almost entirely under it, especially in multiparous women. It also determines the presence or absence of symptom of balloting, characteristic of the head. To do this, the palms of both hands are pressed tightly against the lateral sections of the fetal head, then a push is made with the right hand in the region of the right half of the head. In this case, the head is repelled to the left and transmits a push to the left hand .
In cephalic presentation, one should strive to get an idea of the size of the head and the density of the bones of the skull, the location of the occiput, forehead and chin, as well as their relationship to each other.
Using the fourth technique, it is possible to determine the presence or absence of an angle between the back of the head and the back of the fetus (the higher the chin with the head fixed at the entrance, the more pronounced the flexion and the more smoothed the angle between the back of the head and the back, and vice versa, the lower the chin is, the more it is extended head), the position and appearance of the fetus according to where the back of the head, forehead, and chin are facing. For example, the back of the head is turned to the left and anteriorly - the first position, front view; the chin is turned to the left and forward - the second position, rear view, etc.
With cephalic presentation, it is also necessary to determine the depth of the head. At the fourth external obstetric examination, the fingers of both hands make a sliding movement along the head in the direction towards themselves. With a high standing of the fetal head, when it is movable above the entrance, you can bring the fingers of both hands under it and even move it away from the entrance (Fig. 6.14, a). If at the same time the fingers diverge, the head is located at the entrance to the small pelvis with a small segment (Fig. 6.14, b). If the hands sliding along the head converge, then the head is either located in a large segment at the entrance, or passed through the entrance and descended into deeper sections (planes) of the pelvis (Fig. 6.14, c). If the fetal head is located in the pelvic cavity so low that it completely fulfills it, then it is usually not possible to probe the head with external methods.

Auscultation. The heartbeat of the fetus in a pregnant woman and a woman in labor is usually listened to with an obstetric stethoscope. His wide funnel is applied to the woman's stomach.

Auscultation reveals fetal heart sounds. In addition, you can catch other sounds emanating from the mother's body: the beating of the abdominal aorta, coinciding with the woman's pulse; "blowing" uterine noises that occur in large blood vessels passing along the side walls of the uterus (coincide with the woman's pulse); irregular bowel sounds. Fetal heart sounds give an idea of the condition of the fetus.
Fetal heart sounds are heard from the beginning of the second half of pregnancy and become clearer every month. They are heard from the side of the back of the fetus, and only with facial presentation, the heartbeat of the fetus is more clearly heard from the side of its chest. This is due to the fact that with facial presentation, the head is maximally extended and the breast is adjacent to the wall of the uterus closer than the back.
With occipital presentation, the heartbeat is well heard below the navel on the left in the first position, on the right - in the second (Fig. 6.16). In breech presentation, the heartbeat is heard at or above the navel.

In transverse positions, the heartbeat is heard at the level of the navel closer to the fetal head.
In multiple pregnancies, the fetal heartbeat is usually clearly heard in different parts of the uterus.
During childbirth, when the fetal head is lowered into the pelvic cavity and its birth, the heartbeat is better heard closer to the symphysis, almost along the midline of the abdomen.
ADDITIONAL EXAMINATION METHODS IN OBSTETRICS AND PERINATOLOGY
Assessment of fetal cardiac activity. Cardiac activity is the most accurate and objective indicator of the state of the fetus in the ante- and intranatal periods. For its assessment, auscultation with an obstetric stethoscope, electrocardiography (direct and indirect), phonocardiography and cardiotocography are used.
Indirect electrocardiography carried out by applying electrodes to the anterior abdominal wall of the pregnant woman (the neutral electrode is located on the thigh). Normally, the ventricular complex is clearly visible on the electrocardiogram (ECG). QRS, sometimes prong R. Maternal complexes are easy to differentiate with simultaneous recording of the mother's ECG. The fetal ECG can be recorded from the 11-12th week of pregnancy, but it can be recorded in 100% of cases only by the end of the third trimester. As a rule, indirect electrocardiography is used after 32 weeks of pregnancy.
Direct electrocardiography is performed by applying electrodes to the fetal head during childbirth with the opening of the cervix by 3 cm or more. An atrial wave is noted on a direct ECG. R, ventricular complex QRS and prong T.
When analyzing the antenatal ECG, the heart rate, rhythm, size and duration of the ventricular complex, as well as its shape are determined. Normally, the rhythm of the heartbeat is correct, the heart rate ranges from 120 to 160 minutes, the tooth R pointed, the duration of the ventricular complex is 0.03-0.07 s, the voltage is 9-65 μV. With increasing gestational age, the voltage gradually increases.
Phonocardiogram(FCG) of the fetus is recorded when a microphone is applied at the point of best listening to its heart sounds with a stethoscope. It is usually represented by two groups of oscillations that reflect I and II heart sounds. Sometimes III and IV tones are registered. The duration and amplitude of heart sounds fluctuate markedly in the third trimester of pregnancy, on average, the duration of the first tone is 0.09 s (0.06-0.13 s), the second tone is 0.07 s (0.05-0.09 s) .
With simultaneous registration of ECG and FCG of the fetus, it is possible to calculate the duration of the phases of the cardiac cycle: phases of asynchronous contraction (AC), mechanical systole (Si), total systole (So), diastole (D). The phase of asynchronous contraction is detected between the beginning of the tooth Q and I tone, its duration is 0.02-0.05 s. Mechanical systole is the distance between the beginning of I and II tone and lasts from 0.15 to 0.22 s.
The general systole includes a mechanical systole and an asynchronous contraction phase. Its duration is 0.17-0.26 s. Diastole is calculated as the distance between the beginning of II and I tone, its duration is 0.15-0.25 s. The ratio of the duration of total systole to the duration of diastole at the end of an uncomplicated pregnancy averages 1.23.
Despite the high information content, the methods of fetal electrocardiography and phonocardiography are laborious, and the analysis of the data obtained takes a long time, which limits their use for a quick assessment of the fetal condition. In this regard, at present, cardiotocography is widely used in obstetric practice (from the 28-30th week of pregnancy).
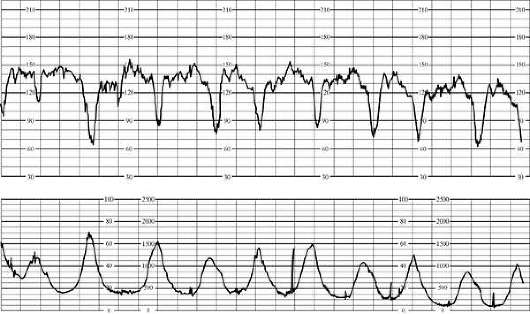
Cardiotocography. There are indirect (external) and direct (internal) cardiotocography. During pregnancy, only indirect cardiotocography is used; at present, it is also used in childbirth, since the use of external sensors has practically no contraindications and does not cause any complications (Fig. 6.17).

An external ultrasonic sensor is placed on the anterior abdominal wall of the mother in the place of the best audibility of the fetal heart sounds, an external strain gauge is applied in the area of the uterine fundus. When using the internal registration method during childbirth, a special spiral electrode is fixed on the skin of the fetal head.
The study of the cardiotocogram (CTG) begins with the determination of the basal rhythm (Fig. 6.18). The basal rhythm is understood as the average value between the instantaneous values of the fetal heartbeat, which remains unchanged for 10 minutes or more; at the same time, acceleration and deceleration are not taken into account.

When characterizing the basal rhythm, it is necessary to take into account its variability, i.e. the frequency and amplitude of instantaneous changes in the fetal heart rate (instantaneous oscillations). The frequency and amplitude of instantaneous oscillations are determined for each subsequent 10 minutes. The amplitude of the oscillations is determined by the magnitude of the deviation from the basal rhythm, the frequency is determined by the number of oscillations in 1 min.
In clinical practice, the following classification of types of basal rate variability is most widely used:
Silent (monotone) rhythm with low amplitude (0.5 per minute);
Slightly undulating (5-10 per minute);
Undulating (10-15 per minute);
Saltatory (25-30 per minute).
Variability in the amplitude of instantaneous oscillations can be combined with a change in their frequency.
The recording is carried out in the position of the woman on the left side for 40-60 minutes.
To unify and simplify the interpretation of antenatal CTG data, a scoring system has been proposed (Table 6.1).
Table 6.1. Prenatal Fetal Cardiac Assessment Scale
A score of 8-10 points indicates the normal state of the fetus, 5-7 points - indicates the initial signs of a violation of his life, 4 points or less - serious changes in the state of the fetus.
In addition to the analysis of fetal cardiac activity at rest, using cardiotocography, it is possible to assess the reactivity of the fetus during pregnancy by changing its cardiac activity in response to spontaneous movements. This is a non-stress test (NST) or a stress test for the administration of oxytocin to the mother, a short breath-hold on inhalation or exhalation, thermal stimulation of the skin of the abdomen, physical activity, stimulation of the nipples or acoustic stimulation.
It is advisable to start the study of fetal cardiac activity with the use of NBT.
Nestreccotest. The essence of the test is to study the reaction of the fetal cardiovascular system to its movements. NST is called reactive if two increases in the fetal heart rate or more are observed within 20 minutes, at least 15 per minute and lasting at least 15 s, associated with fetal movements (Fig. 6.19). NBT is considered unresponsive for less than two fetal heart rate increases of less than 15 beats per minute for less than 15 seconds for 40 minutes.

Oxytocin test(contractile stress test). The test is based on the response of the fetal cardiovascular system to induced uterine contractions. A woman is injected intravenously with a solution of oxytocin containing 0.01 IU in 1 ml of isotonic sodium chloride solution or 5% glucose solution. The test can be evaluated if at least three uterine contractions are observed within 10 minutes at an infusion rate of 1 ml / min. With sufficient compensatory capabilities of the fetoplacental system, in response to uterine contraction, a mildly pronounced short-term acceleration or early short-term deceleration is observed.
Contraindications to the oxytocin test: pathology of placenta attachment and its partial premature detachment, threatened miscarriage, uterine scar.
When determining the state of the fetus in childbirth, CTG evaluates the basal rhythm of the heart rate, the variability of the curve, as well as the nature of slow accelerations (accelerations) and decelerations (decelerations) of the heart rate, comparing them with data reflecting the contractile activity of the uterus.
Depending on the time of occurrence relative to uterine contractions, four types of decelerations are distinguished: dip 0, dip I, dip II, dip III. The most important parameters of decelerations are the duration and amplitude of the time from the onset of contraction to the onset of slowdown. In the study of the time relationships of CTG and histograms, early (the beginning of the decrease in heart rate coincides with the onset of the contraction), late (30-60 s after the onset of uterine contraction), and decreases outside the contraction (after 60 s or more) are distinguished.
Dip 0 usually occurs in response to uterine contractions, less often sporadically, lasts 20-30 seconds and has an amplitude of 30 per minute or more. In the second stage of labor, it has no diagnostic value.
Dip 1 (early deceleration) is a reflex reaction of the fetal cardiovascular system to compression of the head or umbilical cord during contraction. Early deceleration begins simultaneously with a contraction or with a delay of up to 30 seconds and has a gradual beginning and end (Fig. 6.20). The duration and amplitude of decelerations correspond to the duration and intensity of the contraction. Dip 1 is equally common in physiological and complicated births.
Dip II (late deceleration) is a sign of impaired uteroplacental circulation and progressive fetal hypoxia. Late deceleration occurs in connection with the contraction, but is significantly delayed - up to 30-60 s from its onset. The total duration of decelerations is usually more than 1 min. There are three degrees of severity of decelerations: mild (decreasing amplitude up to 15 per minute), medium (16-45 per minute) and severe (more than 45 per minute). In addition to the amplitude and total duration of late deceleration, the severity of the pathological process reflects the time of recovery of the basal rhythm. V-, U- and W-shaped decelerations are distinguished by shape.
Dip III is called variable deceleration. Its appearance is usually associated with the pathology of the umbilical cord and is explained by stimulation of the vagus nerve and secondary hypoxia. The amplitude of variable decelerations ranges from 30 to 90 per minute, and the total duration is 30-80 seconds or more. Decelerations are very diverse in form, which greatly complicates their classification. The severity of variable decelerations depends on the amplitude: mild - up to 60 per minute, moderate - from 61 to 80 per minute and severe - more than 80 per minute.
In practice, the most convenient assessment of the state of the fetus is the time of delivery on the scale proposed by G.M. Savelieva (1981) (Table 6.2).
Table 6.2. The scale for assessing the cardiac activity of the fetus during childbirth (Saveleva G.M., 1981)
Period childbirth | Options cardiac activities | Norm | Initial signs hypoxia | Expressed signs hypoxia |
Basal heart rate | Bradycardia (up to 100) Tachycardia (no more than 180) | Bradycardia (less than 100) |
||
Instant fluctuations in heart rate (ICHR) | Periodic monotonicity (0-2) | Persistent monotony (0-2) |
||
Reaction to the fight | Is absent; increase in the amplitude of the MCHR; early slowdowns | Short-term late slowdowns | Long late slowdowns |
|
Bradycardia | Bradycardia (less than 100 with a progressive drop in frequency); tachycardia (more than 180) |
|||
Periodic monotonicity | monotone; pronounced arrhythmia |
|||
Reaction to push | Early slowdowns (up to 80 per minute); W-shaped variable slowdowns (up to 75-85 per minute); short-term increases (up to 180 per minute) | Late slowdowns (up to 60 per minute); W-shaped variable slowdowns (up to 60 per minute) | Long late reductions (up to 50 in a minute); long-term W-shaped variable slowdowns (up to 40 per minute) |
When using cardiotocography during childbirth, a constant assessment of the fetal cardiac activity throughout their entire length is necessary.
Ultrasound scanning (sonography). Ultrasound examination (ultrasound) is currently the only highly informative, harmless and non-invasive method that allows you to objectively monitor the development of the embryo from the earliest stages and dynamically monitor the condition of the fetus. The method does not require special preparation of the pregnant woman. In obstetric practice, transabdominal and transvaginal scanning is used.
Establishing pregnancy and assessing its development in the early stages are the most important tasks of ultrasound diagnostics in obstetrics (Fig. 6.21).

Diagnosis of uterine pregnancy with ultrasound is possible from the earliest possible date. From the 3rd week, a fetal egg begins to be visualized in the uterine cavity in the form of an echo-negative formation of a rounded or ovoid shape with a diameter of 5-6 mm. At 4-5 weeks, it is possible to identify an embryo - an echopositive strip 6-7 mm in size. The head of the embryo is identified from 8-9 weeks in the form of a separate anatomical formation of a rounded shape with an average diameter of 10-11 mm.
The most accurate indicator of the gestational age in the first trimester is the coccyx-parietal size (KTR) (Fig. 6.22). When the embryo is not yet visible or is difficult to detect, it is advisable to use the average internal diameter of the fetal egg to determine the gestational age.

The assessment of the vital activity of the embryo in the early stages of gestation is based on the registration of its cardiac activity and motor activity. With ultrasound, it is possible to record the cardiac activity of the embryo from the 4-5th week. The heart rate gradually increases from 150-160 per minute in 5-6 weeks. to 175-185 per minute at 7-8 weeks, followed by a decrease to 150-160 per minute by 12 weeks. Motor activity is detected from 7-8 weeks.
When studying the development of the fetus in the II and III trimesters of pregnancy, the biparietal size and head circumference, the average diameter of the chest, the diameters or circumference of the abdomen, and the length of the femur are measured, while determining the estimated weight of the fetus (Fig. 6.23).



With the use of modern ultrasound equipment, it became possible to evaluate the activity of various organs and systems of the fetus. Most congenital malformations can be diagnosed prenatally. For their detailed assessment, three-dimensional echography is used, which gives a three-dimensional image.
Ultrasound makes it possible to accurately determine the location, thickness and structure of the placenta. With real-time scanning, especially with transvaginal examination, a clear image of the chorion can be obtained from 5-6 weeks of pregnancy.
An important indicator of the condition of the placenta is its thickness with typical growth as pregnancy progresses. By 36-37 weeks, the growth of the placenta stops. In the future, during the physiological course of pregnancy, the thickness of the placenta decreases or remains at the same level, amounting to 3.3-3.6 cm.
Ultrasound signs of changes in the placenta as pregnancy progresses are determined by the degree of its maturity according to P. Grannum (Table 6.3, Fig. 6.24).




Table 6.3. Ultrasound signs of the degree of maturity of the placenta
Degree placental maturity | Chorionic membrane | Parenchyma | Basal layer |
straight, smooth | homogeneous | Not identified |
|
slightly wavy | Few echo zones | Not identified |
|
with grooves | Linear echogenic seals | Linear arrangement of small echogenic areas (basal dotted line) |
|
With depressions reaching the basal layer | Round seals with depressions in the center | Large and partially merged echogenic areas, giving an acoustic shadow |
Doppler study of blood flow in the mother-placenta-fetus system. There are quantitative and qualitative methods for assessing dopplerograms of blood flow in the studied vessel. Qualitative analysis is widely used in obstetric practice. The main value in this case is not the absolute value of the speed of blood movement, but the ratio of blood flow velocities in systole (C) and diastole (D). The most commonly used are the systolic-diastolic ratio (SDO), the pulsation index (PI), for the calculation of which the average blood flow velocity (CBR) and the resistance index (IR) are additionally taken into account (Fig. 6.25).

The greatest practical value during pregnancy is the study of uteroplacental blood flow: in the uterine arteries, their branches (spiral, arcuate, radial) and the umbilical artery, as well as fetal hemodynamics: in the aorta and cerebral vessels of the fetus. At present, the study of venous blood flow in the fetus in ductus venosus.
During uncomplicated pregnancy, peripheral vascular resistance gradually decreases, which is expressed by a decrease in blood flow indices (Table 6.4).
Table 6.4. Doppler parameters in the fetal aorta, umbilical cord artery and uterine artery in the third trimester of uncomplicated pregnancy, M±m
An increase in vascular resistance, manifested primarily by a decrease in the diastolic component of blood flow, leads to an increase in these indices.
Doppler echocardiography of the fetus is also used in obstetric practice. It has the greatest practical value in the diagnosis of congenital heart defects.
Color Doppler mapping (CDM) is a combination of two-dimensional echo-impulse information and color information about the speed of blood flow in the organs under study. The high resolution of the devices makes it possible to visualize and identify the smallest vessels of the microvasculature. This makes the method indispensable in the diagnosis of vascular pathology, in particular, for the detection of retroplacental bleeding; vascular changes in the placenta (angioma), their anastomoses, leading to reverse arterial perfusion in twins, entanglement of the umbilical cord. In addition, the method allows assessing malformations of the heart and intracardiac shunts (from the right ventricle to the left ventricle through a ventricular septal defect or regurgitation through the valve), identify the anatomical features of the fetal vessels, especially small caliber (renal arteries, circle of Willis in the fetal brain). CDI provides the possibility of studying blood flow in the branches of the uterine artery (up to the spiral arteries), the terminal branches of the umbilical artery, and the intervillous space.
Determination of the biophysical profile of the fetus. Real-time ultrasound devices allow not only to assess the anatomical features of the fetus, but also to obtain fairly complete information about its functional state. Currently, the so-called fetal biophysical profile (BFPP) is used to assess the intrauterine state of the fetus. Most authors include in this concept the data of a non-stress test and indicators determined by ultrasound scanning in real time: respiratory movements, motor activity, fetal tone, amniotic fluid volume, degree of placental maturity (Table 6.5).
Options | 2 points | 1 point | 0 points |
Non-stress test | 5 or more accelerations with an amplitude of at least 15 per minute and a duration of at least 15 s, associated with fetal movements for 20 minutes | From 2 to 4 accelerations with an amplitude of at least 15 per minute and a duration of at least 15 s, associated with fetal movements in 20 minutes | 1 acceleration or less in 20 minutes |
Fetal activity | At least 3 generalized movements within 30 minutes | 1 or 2 generalized fetal movements within 30 minutes | Absence of generalized fetal movements within 30 minutes |
Fetal respiratory movements | At least 1 episode of respiratory movements lasting at least 60 seconds in 30 minutes | At least 1 episode of respiratory movements lasting from 30 to 60 seconds in 30 minutes | No breathing or breathing less than 30 seconds in 30 minutes |
Muscle tone | 1 episode of return of fetal limbs from extended to flexed position or more | At least 1 episode of the return of the fetal limbs from extended to flexed position | Limbs in extended position |
Amount of amniotic fluid | Vertical pocket of a free area of water 2-8 cm | 2 pockets or more of amniotic fluid 1-2 cm in size | Amniotic fluid pocket less than 1 cm |
maturity placenta | Corresponds to gestational age | III degree of maturity up to 37 weeks |
The high sensitivity and specificity of BFPP are explained by a combination of markers of acute (non-stress test, respiratory movements, motor activity and fetal tone) and chronic (amniotic fluid volume, degree of placental maturity) fetal disorders. Reactive NST, even without additional data, indicates a satisfactory condition of the fetus, with non-reactive NST, ultrasound of other biophysical parameters of the fetus is indicated.
Determination of BFPP is possible already from the beginning of the III trimester of pregnancy.
Ultrasound examination of the brain (neurosonography) of a newborn. Indications for neurosonography in the early neonatal period are chronic oxygen deficiency in the prenatal period of development, birth in breech presentation, operative delivery, rapid and rapid delivery, asphyxia, as well as high or low birth weight, neurological symptoms.
The study is carried out using sectoral sensors (3.5-7.5 MHz). Special medical preparation is not required. The duration of the study is on average 10 minutes.
In an echographic examination of the brain, standard sections are sequentially obtained in the coronal and sagittal planes through the large fontanel (Fig. 6.26). Scanning through the temporal bone of the child's head allows a better assessment of the state of the extracerebral spaces. Cerebral blood flow in children is determined mainly in the anterior and middle cerebral arteries. Arteries appear on the screen as pulsating structures. Visualization is greatly facilitated by the use of color Doppler. When analyzing the curves of blood flow velocities in the cerebral vessels, the systolic-diastolic ratio and the resistance index are determined.

With neurosonography, it is possible to diagnose cerebral ischemia and edema, changes in the ventricular system of the brain, intracranial hemorrhages of various localization and severity, and malformations of the central nervous system.
Examination of amniotic fluid includes determination of quantity, color, transparency, biochemical, cytological and hormonal composition.
Determining the amount of amniotic fluid. Determining the volume of amniotic fluid with ultrasound can be subjective or objective. An experienced specialist can assess the amount of amniotic fluid with careful longitudinal scanning (a large amount of fluid between the fetus and the anterior abdominal wall of a pregnant woman with polyhydramnios, a sharp decrease in the number of spaces free from echostructures with oligohydramnios).
There are objective semi-quantitative echographic criteria for the non-invasive assessment of the amount of amniotic fluid. To do this, measure the depth of the free area of the amniotic fluid (vertical pocket), the value of which is normally from 2 to 8 cm. uterus. In a normal pregnancy, the IAI is 8.1-18 cm.
Amnioscopy- transcervical examination of the lower pole of the fetal bladder. During amnioscopy, attention is paid to the color and consistency of amniotic fluid, the admixture of meconium or blood, the presence and mobility of flakes of caseous lubricant. Indications for amnioscopy are suspicion of chronic fetal hypoxia, post-pregnancy, isoserological incompatibility of maternal and fetal blood. For amnioscopy, the pregnant woman is placed in a gynecological chair and a vaginal examination is performed to determine the patency of the cervical canal. Under aseptic conditions, a tube with a mandrel is inserted into the cervical canal through the finger or after the neck is exposed by mirrors. The diameter of the tube is selected depending on the opening of the neck (12-20 mm). After removing the mandrin and turning on the illuminator, the tube is positioned in such a way that the presenting part of the fetus is visible, from which the light beam is reflected. If the mucus plug interferes with the examination, it is carefully removed with a tupfer. With a low location of the placenta on the fetal membranes, a vascular pattern is clearly visible. Contraindications to amnioscopy: inflammatory processes in the vagina and cervix, placenta previa.
Amniocentesis- an operation, the purpose of which is to obtain amniotic fluid for biochemical, hormonal, immunological, cytological and genetic studies. The results allow us to judge the condition of the fetus.
Indications for amniocentesis are isoserological incompatibility of maternal and fetal blood, chronic fetal hypoxia (pregnancy prolongation, preeclampsia, extragenital diseases of the mother, etc.), determination of the degree of fetal maturity, antenatal diagnosis of its sex, the need for karyotyping in cases of suspected congenital or hereditary pathology of the fetus , microbiological research.
Depending on the puncture site, there are transvaginal and transabdominal amniocentesis. The operation is performed under ultrasound guidance, choosing the most convenient puncture site depending on the location of the placenta and small parts of the fetus (Fig. 6.27).

During transabdominal amniocentesis, after treatment of the anterior abdominal wall with an antiseptic, anesthesia of the skin, subcutaneous tissue and subaponeurotic space is performed with a 0.5% solution of novocaine. For research take 10-15 ml of amniotic fluid. In Rh-sensitized pregnant women, when a bilirubin optical density (OPD) study is necessary, the amniotic fluid sample should be quickly transferred to a dark vessel to avoid changing the properties of bilirubin under the influence of light. Samples contaminated with blood or meconium are unsuitable for research.
Transvaginal amniocentesis is performed through the anterior vaginal fornix, cervical canal, or posterior vaginal fornix. The choice of the insertion site for the puncture needle depends on the location of the placenta. After sanitation of the vagina, the cervix is fixed with bullet forceps, shifted up or down, depending on the method chosen, and the vaginal wall is punctured at an angle to the wall of the uterus. When the puncture needle enters the uterine cavity, amniotic fluid begins to stand out from its lumen.
Complications that are possible with amniocentesis: premature rupture of amniotic fluid (more often with transcervical access), injury to the fetal vessels, injury to the bladder and intestines of the mother, chorioamnionitis. Complications of amniocentesis can also include premature rupture of membranes, preterm labor, placental abruption, fetal injury, and umbilical cord injury. However, due to the widespread introduction of ultrasound guidance during this operation, complications are extremely rare. In this regard, the contraindications to amniocentesis have also changed: the threat of abortion remained practically the only contraindication to it. Amniocentesis, like all invasive interventions, is performed only with the consent of the pregnant woman.
Determining the degree of maturity of the fetus. For this purpose, a cytological examination of the amniotic fluid is carried out. To obtain and study the sediment, the amniotic fluid is centrifuged at 3000 rpm for 5 minutes, the smears are fixed with a mixture of ether and alcohol, then stained according to the Garras-Shor method, Papanicolaou or, more often, 0.1% Nile blue sulfate solution. Non-nuclear lipid-containing cells (a product of the sebaceous glands of the fetal skin) stain orange (so-called orange cells). Their content in the smear corresponds to the maturity of the fetus: up to 38 weeks of gestation, the number of these cells does not exceed 10%, and after
38 weeks reaches 50%.
To assess the maturity of the lungs of the fetus, the concentration of phospholipids in the amniotic fluid is also determined, primarily the ratio of lecithin / sphingomyelin (L / C). Lecithin, saturated with phosphatidylcholine, is the main active principle of the surfactant. Interpretation of the value of the ratio L/S:
L / S \u003d 2: 1 or more - light mature. Only 1% of newborns are at risk of developing respiratory distress syndrome;
L / S = 1.5-1.9: 1 - development of respiratory distress syndrome is possible in 50% of cases;
L / S = less than 1.5: 1 - development of respiratory distress syndrome is possible in 73% of cases.
The method of qualitative assessment of the ratio of lecithin and sphingomyelin (foam test) has also found practical application. For this purpose, 3 ml of ethyl alcohol is added to a test tube with 1 ml of amniotic fluid and within
Shake the tube for 3 minutes. The resulting ring of foam indicates the maturity of the fetus (positive test), the absence of foam (negative test) indicates the immaturity of the lung tissue.
Diagnosis of outflow of amniotic fluid. One of the methods for diagnosing the outflow of amniotic fluid during pregnancy is a cytological examination of fresh stained preparations. A drop of vaginal contents is applied to a glass slide, a drop of 1% eosin solution is added and covered with a coverslip. Under a microscope on a pink background, brightly colored epithelial cells of the vagina with nuclei, erythrocytes, leukocytes are visible. When the waters have broken, large accumulations of uncolored "scales" of the skin of the fetus are visible.
In recent years, in order to diagnose prenatal rupture of amniotic fluid, the amnio test is widely used - special swabs soaked in a reagent that change color when in contact with amniotic fluid.
X-ray examination. Due to the negative impact of ionizing radiation on the embryo and fetus, X-ray examination is rarely used. At the end of pregnancy, the radiosensitivity of the fetus decreases, X-ray studies at this time are less dangerous. In obstetric practice, to clarify changes in the bone pelvis, X-ray pelvimetry is sometimes used, which allows you to determine the shape and true dimensions of the small pelvis.
Indications for X-ray pelviometry: suspicion of mismatch between the size of the pelvis of the mother and the head of the fetus, anomalies in the development of the pelvis, spinal injuries.
Produce direct and lateral pictures of the pelvis. On a radiograph taken in direct projection, the transverse size of the pelvis and the fronto-occipital size of the head are measured. On the lateral radiograph, the true conjugate and the large transverse size of the head are determined. The shape and dimensions of the sacrum on the radiograph are characterized by the length of its chord, the angle of the sacral curvature and the magnitude of its radius. To assess the sacrum, the sacral index is used, which is calculated as the ratio of the length of the chord of the sacrum to the radius of the sacral curvature. The sacral index reflects the length of the sacrum and the severity of its curvature. The definition of flattening of the sacrum is an important feature for predicting the nature of the birth act.
X-ray pelviometry data allow you to clarify the shape of the narrow pelvis and accurately determine the degree of narrowing.
Determination of tissue pO 2in the fetus. Oxygen tension (pO2) in the tissues of the fetus can be determined by the polarographic method during childbirth in the absence of a fetal bladder. This provides an early diagnosis of intrauterine fetal hypoxia. You can apply the intra- and transdermal polarographic method. For intradermal determination of pO2, open microelectrodes are used, which are easily and without complications introduced into tissues. Interstitial polarographic determination has a well-known advantage, since the electrodes respond faster to changes in pO2 and have less inertness than electrodes for transcutaneous measurement.
The working needle electrode is inserted under the skin of the fetal head to a depth of 0.5-0.6 mm after the outflow of amniotic fluid and the opening of the cervix to
4 cm or more, the reference electrode is inserted into the posterior fornix of the vagina.
Study of the blood of the fetus and newborn. The most important information about the condition of the fetus can be given by the results of a direct study of its blood obtained from the umbilical cord or head.
Cordocentesis. Blood is obtained from the vein of the umbilical cord by intrauterine puncture under ultrasound control (Fig. 6.28).

The method is indicated for diagnosing congenital and hereditary pathologies (fetal karyotyping), intrauterine infection, fetal hypoxia, its anemia during immunoconflict pregnancy. In addition to a wide range of diagnostic tasks, cordocentesis also allows solving some important problems of intrauterine therapy in fetal hemolytic disease.
Cordocentesis is performed after 18 weeks of pregnancy. Before taking the blood of the fetus, the localization of the placenta and the place of origin of the umbilical cord are established. When the placenta is located on the anterior wall of the uterus, the needle for blood aspiration is carried out transplacentally, in the case of localization of the placenta on the posterior wall, the needle is inserted transamnionally. The umbilical cord is punctured near the place of its discharge from the placenta. With high motor activity of the fetus, which interferes with the puncture, intramuscular or intravenous administration of drugs to the fetus is recommended to ensure its short-term complete immobilization. To do this, use the muscle neuroblocker pipecuronium (arduan) at a dose of 0.025-0.25 mg/kg. The volume of the blood sample depends on the indication for cordocentesis; usually no more than 2 ml is required.
The risk of complications during cordocentesis for a pregnant woman is low. Complications for the fetus include premature outflow of water (0.5%), bleeding from a punctured vessel (5-10%), as a rule, not prolonged and not life-threatening for the fetus. Perinatal losses do not exceed 1-3%. Contraindications for cordocentesis are the same as for amniocentesis.
Determination of the acid-base state (CBS) of the blood. During childbirth, capillary blood from the fetus is obtained from the presenting part according to the Zaling method. For this purpose, after the outflow of amniotic fluid, a metal amnioscope tube with fiber optics is inserted into the birth canal. At the same time, the area of the presenting part of the head or buttock is clearly visible, the skin of which is wiped with a gauze swab in order to create hyperemia. A special scarifier is used to puncture the skin to a depth of 2 mm, after which blood is collected (except for the first drop) in a sterile heparinized polyethylene capillary without air layers and amniotic fluid impurities. The study of blood microdoses allows you to quickly obtain information about the state of the fetus, but the method is very laborious and not always feasible.
To determine the CBS of blood in a newborn, blood is taken from the vessels of the umbilical cord immediately after birth or capillary blood is used from the heel of the child.
In the study of CBS of blood, the value of pH, BE (deficiency of bases or excess of acids), pCO2 (partial tension of carbon dioxide), pO2 (partial tension of oxygen) are taken into account.
Biopsy (aspiration) of chorionic villi - an operation, the purpose of which is to obtain chorionic villous cells for fetal karyotyping and determination of chromosomal and gene anomalies (including the determination of hereditary metabolic disorders), as well as to determine the sex of the fetus. Samples are taken transcervically or transabdominally at 8-12 weeks of gestation under ultrasound control. A sterile polyethylene flexible catheter 26 cm long and 1.5 mm in outer diameter is inserted into the uterine cavity and carefully advanced under visual control to the placenta localization site and further between the uterine wall and placental tissue. Then, with a syringe with a capacity of up to 20 ml, containing 3-4 ml of nutrient medium and heparin, chorionic tissue is aspirated, which is then examined (Fig. 6.29). You can take samples of chorionic tissue in multiple pregnancies.

Complications of chorionic villus biopsy are intrauterine infection, bleeding, spontaneous miscarriage, and hematoma formation. Late complications include premature birth, low birth weight of newborns (less than 2500 g), fetal malformations. Perinatal mortality reaches 0.2-0.9%. Contraindications for chorionic biopsy may include genital tract infection and symptoms of threatened miscarriage. Placentocentesis may be performed later in pregnancy.
Fetoscopy(direct examination of the fetus) is used to detect congenital and hereditary pathologies. The method allows you to examine parts of the fetus through a thin endoscope inserted into the amniotic cavity, and through a special channel to take blood and epidermis samples for examination. Fetoscopy is carried out as one of the final stages of the examination in cases of suspected congenital anomalies of the fetus.
Fetoscope insertion technique: after appropriate treatment of the skin under local anesthesia under sterile conditions, a small skin incision is made and the trocar, located in the cannula, is inserted into the uterine cavity. Then it is removed, a sample of amniotic fluid is obtained for examination, an endoscope is inserted into the cannula and a targeted examination of the fetus is carried out. If necessary, take a blood sample or biopsy of the skin of the fetus. At the end of the operation, cardiomonitoring of the fetus is carried out; the pregnant woman remains under observation for 24 hours.
Complications of fetoscopy include rupture of amniotic fluid, termination of pregnancy. Complications such as bleeding and the development of infection, the formation of small superficial hematomas on the limbs of the fetus, are extremely rare. Due to the possibility of termination of pregnancy, fetoscopy is rarely used.
Study of the hormonal profile. Biological methods for diagnosing pregnancy, based on the reaction of animals to the administration of the patient's urine, containing or not containing XE, have now lost their leading role. Preference is given to immunological methods.
Immunological methods for diagnosing pregnancy. Immunological methods include various methods for determining chorionic gonadotropin (CG) or its b-subunit (b-CG) in blood serum and urine. Preference is given to the radioimmunological method for the quantitative determination of b-CG in blood serum, since it has a high specificity and sensitivity. Enzyme immunoassay methods for detecting hCG in the urine, as well as other variants of immunological tests (capillary, plate) deserved a positive assessment. Have the right to exist and such well-known serological methods for determining hCG in the urine, such as the reaction of inhibition of agglutination of erythrocytes or the deposition of latex particles.
Agglutination, or latex particle fixation test, is a method for determining the level of hCG in the urine, which is excreted in the urine 8 days after fertilization. A few drops of the patient's urine are mixed with CG antibodies, then CG-coated latex particles are added. If hCG is present in the urine, it binds to antibodies; if hCG is absent, then the antibodies bind to the latex particles. This rapid test is positive in 95% of cases, starting from the 28th day after fertilization.
radioimmunoassay test. The content of the b-subunit of hCG in the blood plasma is determined.
It shows convincing two stripes, and you, carefully listening to yourself, find at least five more signs of pregnancy. There are so many joyful, pleasant minutes ahead, and so many fantasies in my head. But there is still a lot of trouble ahead, the lion's share of which falls on visiting doctors' offices. Of course, going through numerous studies and taking tests is not the most pleasant experience. This is especially true of the examination on the gynecological chair.
More than once I happen to be a witness to a conversation between future and accomplished mothers on the topic of how many times I had to undergo this examination during pregnancy. Some are proud that it was literally a couple of times, others lament that not even a week passed without this procedure. Where is the golden mean? It’s worth mentioning right away that we will talk about the tradition of observing pregnant women in the conditions of a domestic antenatal clinic. Ignorance breeds distrust. Distrust breeds fear. This article is an attempt to break this vicious circle and answer the main questions. How, when and why a pregnant woman is examined on a chair.
Getting ready for inspection
Be prepared for the fact that you will be examined on a chair during your first visit to the gynecologist for pregnancy. In order for the examination to bring a minimum of discomfort and maximum information about your condition, prepare for it at home. In advance, make yourself a calendar on which mark the approximate days on which you would have your period if you had not become pregnant. This is not difficult to do if you have a regular cycle. These days do not plan to visit a doctor, they are considered dangerous, critical periods for the development of pregnancy. For the same reason, if nothing bothers you, postpone all medical examinations and ultrasounds until the eighth week from the first day of your last period.
Before leaving the house, take a shower or bath and put on fresh clothes. At the same time, it is not worth washing especially carefully, and even more so, it is not worth douching, since the doctor must see the state of the vagina in its usual, "everyday" state. Do not use intimate deodorants or perfumes, they often provoke an allergic reaction, which may be regarded by a doctor as inflammation. Should I shave my perineum before visiting the doctor? Of course, it is not very convenient for a doctor to examine a woman with excess hair on the vulva, but if you do not usually do this, then you should not shave, because this can cause severe skin irritation. Empty your bladder. This is necessary in order to evaluate during the examination exactly the sensations of the internal genital organs, and not the filled bladder. The intestines, if possible, should also be empty.
A day before the visit to the doctor, exclude sexual intercourse, as a small amount of seminal fluid often remains in the vagina, which prevents reliable tests. If you are sitting in line for a long time at the gynecologist, do not be too lazy to go to the ladies' room when your turn comes up to empty your bladder.
Think over your clothes. The main thing is that you feel comfortable, and you can quickly undress from below or free your chest. Take socks with you so that, having prepared for a gynecological examination, you don’t have to go to the gynecological chair on the cold floor and your own towel, despite the fact that there will probably be unnecessary pieces of paper in the gynecologist’s office. In order not to burden yourself with thoughts about the conscientiousness of sterilizing examination instruments, purchase a disposable gynecological kit. They are quite inexpensive, sold in most pharmacies. It usually includes a plastic mirror for examining the cervix, it is not as cold as ordinary metal instruments, sterile gloves, special sticks or brushes for taking material for analysis, and a disposable diaper (instead of a towel).
Usually, a gynecological examination is invited after a preliminary conversation, pressure measurement, weighing and examination on the couch. If the office has a separate examination room, please leave your shoes in front of the entrance. Check with the doctor or midwife where you can undress, you should not attach your clothes to a sterile table or radiator, you may stumble upon a not very friendly nurse. Undress slowly, the medical staff will fill out the necessary documents during this time. Put on socks, put a diaper or towel on the chair so that it reaches to the edge, but does not hang from it. Climb up the stairs onto the chair itself and lie down on it so that the buttocks are on the very edge of it. Then place your feet on the stands, the slingshots should be in the popliteal fossa. Do not hesitate and do not be embarrassed to ask the gynecologist how to properly sit in the gynecological chair if this design is unfamiliar to you. Put your hands on your chest and try to calm down and relax. You still have to go through it, the better you relax, the more clear your condition will be to the doctor, the faster the examination will end. Do not try to see everything the doctor is doing or help (interfere?) the doctor with your hands, this makes it difficult to examine and exacerbates discomfort, it is better to ask the doctor about everything before or after the examination.
My light, mirror, tell me...
The study begins with an examination of the external genital organs: the doctor assesses the condition of the skin and mucous membrane of the perineum, large and small labia, clitoris and external opening of the urethra. At the same time, the inner surfaces of the thighs are also examined, which makes it possible to identify varicose veins, the presence of areas of pigmentation or rash elements. Be sure to examine the area of the anus, which allows you to immediately identify the presence of hemorrhoids, cracks and some other disorders.
Then the doctor proceeds to examination in the mirrors. This type of examination is aimed primarily at identifying any diseases of the vagina or the condition of the cervix. Mirrors are of two types: folding and spoon-shaped. The folded speculum is inserted in a closed form, then the folds are opened, and the cervix becomes available for inspection. The walls of the vagina are examined with the gradual removal of the mirror from the vagina. When examined with spoon-shaped mirrors, the rear (lower) mirror is first driven, it is placed on the back wall of the vagina and slightly pressed on the perineum; then, parallel to it, an anterior (upper) mirror is inserted, with which the anterior wall of the vagina is raised. The introduction of the mirror is the most unpleasant part of the examination. In order to be less painful, it is better to relax and push on the mirror, open up towards you when you feel that it has touched you. Then it will enter by itself, and you will not even notice it. After inserting a mirror on the cervix, light is directed and examined. During pregnancy, the cervix is bluish, this is one of the signs of pregnancy. This research method also reveals diseases of the cervix and vagina (inflammation, erosion, polyp, cancer). When examining the cervix, pay attention to the presence of redness (spots) on the outer surface of the cervix. This is what they talk about erosion". Many diseases can be hidden under this sign, but only an examination of the cervix using a special microscope - the “colposcope” will help to make an accurate diagnosis. Perhaps the doctor will perform a colposcopy immediately if his office is equipped with this device or appoint another day. In addition, they look at the state of the external pharynx (the opening of the cervical canal). The appearance of this hole, even without further examination, helps to diagnose the threat of interruption even at a very short time. In addition, according to the state of the external pharynx, isthmic-cervical insufficiency. In this case, the canal is ajar, the shape of the pharynx is often incorrect due to ruptures of the cervix in previous births.
Special attention is paid to the nature of the discharge from the cervix. If the discharge is streaked with blood, this always indicates a possible threat of abortion. If the discharge is cloudy, has an unusual smell, this indicates an infection.
What's up for analysis?
The first analysis that is always done when registering during pregnancy is swab for flora. With a special spoon, the doctor "scoops" the substance from the cervical canal, vagina, urethra and applies it to the glass. The extracted material is examined in the laboratory under a microscope. This method can reveal the inflammatory process (by the number of leukocytes), detect some types of infection (fungal, candidiasis, gonorrhea, trichomoniasis, bacterial vaginosis).
A smear for flora is repeated 3-4 times during pregnancy, even if it was absolutely normal. And this is not accidental, because often during pregnancy infections “wake up” that did not make themselves felt for a long time. So, for example, candidiasis (thrush) in pregnant women occurs 2-3 times more often than in others. During this period, the woman's body is rebuilt, the level of female sex hormones rises. The vaginal environment becomes more acidic, which is very "to the taste" of Candida.
At the same time, hormonal changes in the body lead to a local decrease in cellular immunity and leukocyte activity, which also contributes to increased reproduction of the fungus in the genital tract of the expectant mother. The longer the gestation period, the higher the number of microorganisms, so it is in the last trimester that expectant mothers are especially worried about candidiasis. The aggressive environment that forms in the vagina of a pregnant woman with candidiasis, especially with isthmic-cervical insufficiency, can “melt” the lower pole of the fetal bladder and lead to the outflow of amniotic fluid, which means miscarriage or premature birth.
The second required analysis is cytological examination. In a cytological study, the structural features of the cells of the surface and canal of the cervix are studied. A smear for cytological examination is taken with a special tool - a spatula or brush. This analysis is very important for the detection of various oncological diseases at the earliest stages. And during pregnancy - it is simply necessary, because pregnancy aggravates the course of these diseases. Often another cytological smear is taken from the fornix of the vagina. This analysis allows you to assess the hormonal status of a woman, predict the threat of abortion or disturbances in the uteroplacental blood flow.
In recent years, the vast majority of antenatal clinics have screened pregnant women for sexually transmitted infections ( STI). Most often, these tests are not taken on the first visit, but during a second examination on the armchair. The analysis is taken from the cervical and urethra on several glasses or in a test tube, depending on the method of diagnosing infections. If your antenatal clinic does not have the opportunity to do such an analysis, check with your doctor where you can do it and at what stage of pregnancy it is safe. STIs must be treated, as primary placental insufficiency may form, which indirectly leads to fetal hypoxia. Thus, the child can die from a lack of oxygen while still in the mother's stomach.
smart hands
The mirror can finally be taken out. It is necessary to push and open during its removal, then it will pass easily and painlessly. After examination using mirrors, a two-handed vaginal examination is usually performed, which determines the size, position and condition of the uterus, fallopian tubes, and ovaries. First, the doctor spreads the labia majora, and then gently inserts the index and middle fingers of the right hand into the vagina. The doctor puts his left hand on your stomach. Your hands are on your chest, you do not look at the doctor, breathe deeply and calmly. First, the condition of the vagina is assessed: the width of the lumen and the extensibility of the walls, the presence of scars, tumors, partitions, and other pathological conditions that can affect the course of pregnancy and childbirth.
Then the doctor finds the cervix and determines its shape, size, consistency, location. So, during normal pregnancy, the cervix is tilted back, its length is more than two centimeters, it is dense to the touch, and the canal is not passable for a finger. With the threat of termination of pregnancy, the cervix shortens, softens, shifts to the center, the canal opens. It should be noted that it is enough for an experienced doctor to touch the neck to evaluate it. The doctor will not specifically examine the patency of the cervical canal during a premature pregnancy, so as not to provoke a miscarriage or premature birth by their actions. A simple touch on the cervix does not provoke a miscarriage; during normal sexual intercourse, the “load” on this organ is ten times higher than during examination. Information about the state of the cervix, obtained by the doctor at the first examination, is a sample for later comparison. After all, every woman is different. And the fact that for one is a clear sign of the threat of interruption, for the other - the norm.
Next, the uterus is palpated. The size of the uterus most often corresponds exactly to the gestational age, but it can be larger if a woman suffers from uterine fibroids, is carrying a third or fourth pregnancy, expects twins, or less than the term with a combination of pregnancy and certain gynecological diseases. In addition to size, the doctor pays attention to the consistency and shape of the uterus. The uterus during pregnancy is softer than the non-pregnant one, especially the part of the uterus that is close to the cervix (the so-called isthmus) softens. Irregularities in the uterus can be a sign of an abnormal development of the uterus or the presence of fibroids. For a short period of time, the uterus is mobile and occupies a middle position in the small pelvis. If its mobility is limited or it is deviated to the side, then more often it is associated with an adhesive process or an inflammatory disease of the uterine appendages.
After examining the uterus, the doctor will definitely check the appendages - the ovaries and fallopian tubes. In the early stages, this is especially important to exclude ectopic pregnancy. Examination during an ectopic pregnancy is sharply painful. In addition to ectopic pregnancy, an increase in one of the ovaries is often determined due to the corpus luteum (formation that provides hormonal support for early pregnancy). This condition requires re-examination and observation.
At the end of the study, the inner surface of the sacrum, symphysis and side walls of the pelvis are felt. Feeling the pelvis allows you to identify the deformation of its bones and diagnose the anatomical narrowing of the pelvis. This information will become especially necessary in childbirth.
How often?
Pregnancy is a long process and your condition can change significantly over time. Therefore, the study must be repeated periodically. For example, it is possible to recognize isthmic-cervical insufficiency in time only if, during regular visits to the antenatal clinic, the doctor examines the woman on the armchair. This condition is painless, may not affect well-being. With it, the cervix gradually shortens and opens slightly, the lower pole of the fetal egg becomes infected, the fetal membranes lose their strength, amniotic fluid is poured out and a miscarriage occurs. If you have been told such a diagnosis - do not be alarmed, the main thing is to take action in time. The pathology of the cervical canal is "removed" both surgically and conservatively. Which method is right for you, the doctor will determine. Usually, to monitor the condition of the cervix and analyze the smear for flora, the study is carried out at 20, 28, 32, 36 weeks of pregnancy. This is if nothing bothers you, and the initial examination did not reveal any pathology. The doctor is obliged to see you if you complain of abdominal pain or a change in the nature of the discharge. In addition, after the end of the course of treatment, there should also be a follow-up examination.
Carrying out a certain set of studies in a pregnant woman makes it possible to predict the course of pregnancy and childbirth, possible complications and, therefore, timely correct correction aimed at reducing the risk of developing diseases in her and the fetus. This complex will include: a survey, an objective study of the functions of all organs, external and internal obstetric studies, clinical and laboratory studies.
Survey of a pregnant woman
The collection of anamnesis is carried out according to the following plan.
1. Passport data.
2. Diseases suffered in childhood, adulthood, their course and treatment.
3. Heredity.
4. Working and living conditions.
5. Epidemiological history.
6. Allergological history.
7. Obstetric and gynecological history:
Menstrual function (menarche and the establishment of the menstrual cycle, the duration, pain and regularity of menstruation, the amount of blood lost during menstruation, the date of the last menstruation);
sexual life (at what age, married or not);
Gynecological diseases (what, when, the duration and nature of their course, the therapy performed, the results of treatment);
Generative function - the number of previous pregnancies with a detailed clarification of their course and outcome (artificial and spontaneous abortions, childbirth);
The current pregnancy (the first and second half of pregnancy, previous diseases and for how long, outpatient, inpatient treatment).
Objective research
Examination of a pregnant woman includes: examination of a pregnant woman, special obstetric examination (external and internal), clinical and laboratory studies.
Examination of a pregnant woman includes:
Anthropometric studies (assessment of physique, gait, shape of the abdomen, measurement of height and body weight);
Study of the functions of organs.
Special obstetric study aims to timely assess obstetric factors and resolve the issue of the possibility of conducting labor through the natural birth canal.
External obstetric examination includes the following.
1. Measurement of the circumference of the abdomen and the height of the fundus of the uterus, It is carried out starting from the 16th week of pregnancy at each appearance in the antenatal clinic, which allows you to clarify the correspondence of the height of the fundus of the uterus to the gestational age and timely diagnose polyhydramnios, multiple pregnancy, large fetus, fetal hypotrophy. In the horizontal position of the pregnant woman, the circumference of the abdomen is measured at the level of the navel and the height of the fundus of the uterus from the upper edge of the pubic joint.
2. Measurement of the external dimensions of the large pelvis (allows you to approximately judge the size and shape of the small pelvis) is carried out with a pelvis meter in the following sequence:
Distantia spinarum - the distance between the anterior superior iliac spines (normally 25-26 cm);
Distantia cristarum - the distance between the most distant points of the iliac crests (average is 28-29 cm);
Distantia trochanterica - the distance between the large skewers of the femur (usually 31-32 cm);
Conjugata externa - the distance between the upper edge of the pubic joint and the spinous process of the V lumbar vertebra, measured in the position of the pregnant woman on her side (normally 20-21 cm);
The direct size of the exit of the pelvis (normally 9.5 cm) is the distance between the middle of the lower edge of the pubic joint and the top of the coccyx, measured in the position of the pregnant woman on her back with her legs apart and half-bent at the hip and knee joints;
The transverse size of the outlet of the pelvis (normally 11 cm) is the distance between the inner surfaces of the ischial tubercles (the position of the pregnant woman is the same as when measuring the direct size of the outlet of the pelvis);
Rhombus of Michaelis - assessment of the shape of the rhombus, measurement of the vertical (normally 11 cm) and horizontal (normally 10 cm) of its diagonals (the woman stands with her back to the doctor);
Solovyov's index (gives information about the thickness of the pelvic bones) - the circumference of the wrist joint, which is measured with a centimeter tape (normally 14 cm);
The height of the symphysis (gives an idea of the thickness of the pelvic bones, the measurement is carried out during a vaginal examination).
3. Receptions of Leopold - Levitsky. First reception allows you to determine the height of the fundus of the uterus in relation to the xiphoid process (the height of the fundus of the uterus corresponds to the gestational age) and the part of the fetus that is in the fundus of the uterus. The pelvic end is defined as a large, soft and non-balloting part of the fetus, the head is defined as a large, well-defined, dense balloting part. To do this, place the palms of both hands on the bottom of the uterus and determine the distance between the bottom of the uterus and the xiphoid process or navel, specify the part of the fetus in the bottom of the uterus.
Second reception external obstetric examination is aimed at determining the position, position and type of the fetus.
The position of the fetus is the ratio of the longitudinal axis of the fetus to the longitudinal axis of the uterus. The following positions are distinguished: a) longitudinal - the longitudinal axis of the fetus and the longitudinal axis of the uterus coincide; b) transverse - the longitudinal axis of the fetus crosses the longitudinal axis of the uterus at a right angle; c) oblique - the longitudinal axis of the fetus forms an acute angle with the longitudinal axis of the uterus.
The position of the fetus is the ratio of the back of the fetus to the right and left side of the uterus. In the first position, the back of the fetus (dense and wide surface) faces the left side of the uterus, in the second position, to the right.
View of the fetus - the ratio of the back of the fetus to the anterior (front view) or posterior (posterior view) of the uterine wall.
To perform the second Leopold-Levitsky technique, the palms of both hands of the obstetrician palpate the lateral sections of the uterus, determining the position of the fetus and the location of its back.
Third reception external obstetric examination serves to determine the presenting part of the fetus (head, pelvic end) - To perform it, the obstetrician needs to take the thumb of the right hand as far as possible away from the other four, grasp the presenting part of the fetus and determine its mobility in relation to the plane of entry into the small pelvis.
Fourth reception allows you to determine the level of standing of the presenting part. During pregnancy, the fetal head may be mobile or pressed against the entrance to the small pelvis. This technique is especially important for assessing the progress of the fetal head through the birth canal during childbirth.
4. Auscultation. Fetal heart sounds are heard from the gestational age of 20 weeks in the primiparous and from the 18th week in the multiparous. Auscultation is carried out at each appearance of the pregnant woman in the antenatal clinic, the frequency, rhythm and sonority of the fetal heart tones are assessed (normally, the heartbeat is 120-160 beats / min, clear, rhythmic).
Internal obstetric research carried out when taking a dispensary registration for pregnancy and during hospitalization in the antenatal department with a complicated course of pregnancy or to prepare for childbirth. It is performed in order to assess the condition of the soft birth canal, structural features of the bone pelvis, the nature of the presenting part, as well as to resolve the issue of the method and timing of delivery. The research includes:
Examination and evaluation of the external genital organs (type of pubic hair growth - male or female, correct development of the labia majora and minor, the presence of pathological changes, scars in the vulva and perineum);
Examination using mirrors (valve and spoon-shaped) with an assessment of the shape of the external os of the cervix, the color of the mucous membrane of the vagina and cervix, pathological changes and the nature of the discharge;
Vaginal examination (finger) (according to indications at any stage of pregnancy).
A vaginal examination in the early stages of pregnancy allows you to set the gestational age and identify the pathology of the internal genital organs. In this case, the state is sequentially evaluated:
Vaginas - narrow (in a woman who has not given birth) or capacious (in a woman who has given birth);
Cervix - length, consistency, shape (conical in primiparous and cylindrical in multiparous), the state of the external pharynx (the external pharynx is closed in primiparous and passes the fingertip in multiparous);
Uterus - position, gestational age in weeks, consistency (soft), its mobility and pain on palpation; in the early stages of pregnancy, a ridge-like protrusion on the anterior surface of the uterus along the midline (Genter's sign), asymmetry of the uterus due to the protrusion of one of its corners (Piskachek's sign), contraction and compaction of the uterus on palpation (Snegirev's sign) can be detected;
Adnexa of the uterus (size, consistency, soreness);
Vaults of the vagina (high, free);
bone pelvis (reachability of the cape, pelvic deformities, exostoses).
Vaginal examination during full-term pregnancy makes it possible to establish the degree of readiness of the soft birth canal for childbirth. When performing the study, the state is consistently assessed:
Vagina (narrow or capacious, the presence of pathological changes);
The cervix with the determination of the degree of its "maturity" (Table 1);
The fetal bladder (its presence or absence); presenting part and its relation to the planes of the pelvis;
the oblique pelvis - the height of the symphysis, the presence of bony protrusions and deformities, the shape and depth of the sacral cavity, the reachability of the cape and the measurement of the diagonal conjugate (normally the cape is not reached).
Prenatal care is a careful, systematic examination of pregnant women in order to achieve the best results for the health of the mother and fetus.
The concept of prenatal care (examinations)
The purpose of the prenatal examination is:
1) prevention, screening and elimination of possible complications for the mother and fetus, including socio-economic, emotional, general medical and obstetric factors;
2) education of patients in physiology and pathology, childbirth, postpartum and early neonatal period; recommendations for improving maternal and child health;
3) ensuring adequate psychological support from the doctor, partner and family, especially in the case of the first pregnancy.
So, prenatal care should begin in the preconception period (preconception care) and end one year after birth.
Prenatal care includes a systematic outpatient examination of a pregnant woman, which is carried out according to a well-defined plan and includes screening tests to detect any deviations from the physiological course of pregnancy.
prenatalcare includes:
- Detailed clarification of the complaints of the pregnant woman and a thorough history taking, identification of high risk factors for diseases existing before pregnancy and, if necessary, consultations of related specialists;
- General objective clinical and laboratory examination of pregnant women; body weight control;
- External obstetric examination;
- Internal obstetric examination;
- Prenatal examination of the condition of the fetus, identification of possible complications;
- Recommendations on hygiene, regimen, diet during pregnancy;
- Preparation for childbirth.
First visit of a pregnant woman
During a pregnant woman's first visit to the doctor, a complete life history and standard clinical and laboratory tests should be performed. Preferably, this visit should take place between the 6th and 10th weeks of pregnancy.
Anamnesis. When collecting complaints, they find out the date of the last one, the features of the course of this pregnancy. The patient is asked about symptoms that may indicate any complications of pregnancy: vaginal discharge, vaginal bleeding, leakage, dysuric symptoms. After 20 weeks of pregnancy, the nature of fetal movements and uterine contractions is ascertained.
The obstetric history includes data on the presence and course of previous pregnancies (year, the result of pregnancy - spontaneous (spontaneous) or medical abortion, or childbirth, the term of abortion or childbirth, the characteristics of the course of previous pregnancies, abortions and childbirth, the presence of sexually transmitted diseases, operations, injuries, ectopic pregnancy, multiple pregnancy, data on the type of delivery, the duration of the periods of labor, the weight of children at birth (fetal growth retardation, low birth weight, macrosomia - fetal weight> 4000 g), the presence of complications (hypertension, preeclampsia, premature detachment or placenta previa, postpartum hemorrhage and inflammatory diseases)).
General history includes clarification of social, marital status, heredity, the presence of bad habits (alcohol, tobacco, drugs, drug abuse), domestic violence, chronic extragenital diseases, surgical operations, complications of anesthesia that may affect the course of pregnancy. All data are clearly recorded in the medical documentation (individual map of the pregnant woman and / or birth history).
objectivesurvey. An exceptionally complete objective physical examination of the pregnant woman is carried out (body weight, height, examination of the skin, sclera, oral cavity, throat, mammary glands, detection of edema, varicose veins, determination of body temperature, pulse, blood pressure, heart and lungs, palpation of the abdomen).
The gestational age of the fetus and the expected date of delivery are determined. At the first visit, pregnant women are examined by a therapist, dentist, otolaryngologist, ophthalmologist, dermatovenereologist, and, if necessary, other specialists.
During a gynecological examination, attention is paid to the presence of abnormalities of the vulva, vagina, uterus and appendages, the size of the uterus in weeks of pregnancy, the length, location and consistency of the cervix. Perform a study of the epithelium of the cervix and vaginal microflora. Determine the size of the pelvis (clinical pelvimetry) for pregnant women for the first time and pregnant women again, who had a complicated course of childbirth.
In the second half of pregnancy, the height of the fundus of the uterus above the symphysis is determined (in terms of 18-34 weeks, the height of the uterus above the symphysis in cm corresponds to the gestational age in weeks). If the height of the uterine fundus is 3 cm less than expected for a given gestational age, an ultrasound examination is performed to rule out possible intrauterine growth retardation. After 10-14 weeks, a Doppler study of fetal cardiac activity is used. Auscultation of the fetal cardiac activity is carried out, an external obstetric examination is performed to determine the position, position, type. The tone of the uterus and the nature of its contractions are determined.
External obstetric examination in the III trimester of pregnancy consists of 4 Leopold's maneuvers, which determine the position of the fetus; the presenting part of the fetus and its descent into the pelvis; fetus position:
- I reception - palpation of the fundus of the uterus in the upper quadrant of the abdomen and the determination of the part of the fetus that is located in the fundus of the uterus;
- II reception - palpation of the uterus on the right and left sides of the mother to determine the position of the fetus;
- III reception - palpation of the presenting part of the fetus, the presence of the insertion of the presenting part into the pelvis;
- IV reception - the degree of descent of the presenting part of the fetus into the pelvis is determined.
Laboratorysurvey includes a complete blood count, hemoglobin, glucose, blood typing, Rh factor, biochemical blood test (total protein and fractions, liver tests, coagulogram), syphilis screening (presence of antibodies to rubella, hepatitis B, HIV, chickenpox (in the latter case - in the absence of it in the anamnesis), according to indications - antibodies to toxoplasma, general urinalysis (presence of hematuria, glucosuria, proteinuria, leukocyturia). In doubtful cases, a pregnancy test is performed to confirm pregnancy (presence of hCG). secretions or pain in the lower abdomen determine the level of hCG in the blood serum.
Follow-up visits, as recommended by Asos, should be every 4 weeks until 28 weeks, every 2-3 weeks until 36 weeks, and every week until delivery. For healthy pregnant women who have a low risk of perinatal complications, the following examination periods are recommended: for pregnant women, repeatedly 6-8, 14-16, 24-28, 32, 36, 39 and 41 weeks of gestational age; for pregnant women for the first time - additional visits at 10, 12 and 40 weeks. For high-risk pregnant women, prenatal visits should be individualized and are usually more frequent.
Repeated visits to the pregnant woman to the doctor
In the firsttrimester(during a second visit) find out the symptoms of pregnancy, changes in body weight, take a general blood test, urine. Decreased hematocrit<32% свидетельствует об , увеличение>40% - about hemoconcentration. They advise patients on diet, regimen and hygiene during pregnancy, introduce them to the physiology of pregnancy and childbirth.
In the second trimester, the focus is on genetic screening and the identification of possible anomalies in the development of the fetus, which makes it possible, if necessary, to terminate the pregnancy. Screening for the level of alpha-fetoprotein (AFP) in the mother's blood is usually carried out at 15-18 (15-21) weeks of gestation. An increase in AFP levels (2.5 times higher than the average values) correlates with malformations of the neural tube, anterior abdominal wall, gastrointestinal tract and kidneys of the fetus, as well as non-specific adverse pregnancy outcomes - fetal death, low birth weight, fetal and maternal bleeding); decreased AFP levels - with some forms of aneuploidy, including Down syndrome (trisomy 21), Edwards syndrome (trisomy 18) and Turner syndrome (X0). Screening sensitivity does not increase with simultaneous determination of the level of hCG and estriol in the mother's blood (triple screening).
Genetic amniocentesis or chorionic biopsy, followed by determination of the fetal karyotype, is performed for pregnant women over 35 years of age, and for those who have a high risk of having a child with (1: 270 and above) and structural chromosomal abnormalities.
Between the 18th and 20th weeks, an ultrasound examination (ultrasound) is prescribed to exclude anatomical abnormalities in the development of the fetus, assess the volume of amniotic fluid (amniotic fluid), placental location, and gestational age of the fetus. Assess the contractile function of the uterus, the condition of the cervix (the possibility of premature termination of pregnancy).
In thirdtrimester evaluate the nature of uterine contractions (Braxton-Hicks). With regular contractions, the condition of the cervix is determined (the possibility of premature birth). The frequency of prenatal visits increases from every 2-3 weeks (between 28 and 36 weeks of gestation) to weekly visits after the 36th week of gestational age. Non-immunized patients with Rh-negative blood type at 28 weeks of gestation should be given 1 dose of anti-Rh gamma globulin. After 32-34 weeks of pregnancy, external obstetric examination techniques are used (after Leopold) to identify the position, presentation, position of the fetus, the degree of insertion and the descent of the presenting part of the fetus into the pelvis.
Screening tests for high-risk groups
In the third trimester (27-29 weeks), mandatory screening laboratory tests are performed: complete blood count, biochemical blood test and coagulogram. With a decrease in hemoglobin<110 г / л диагностируют анемию и назначают препараты железа.
To prevent constipation due to the use of iron preparations, pregnant women are also prescribed laxatives (lactulose). The glucose loading test (TGT) is a screening test for gestational diabetes. It consists of taking 50 g of glucose orally, followed by measurement of serum glucose levels 1 hour later. If the glucose level exceeds 14 mmol/l, a glucose tolerance test (TGT) is prescribed. TSH consists of a series of fasting blood glucose measurements and then 100 g of oral glucose. Blood glucose levels are measured 1, 2 and 3 hours after oral administration of glucose. The test is considered positive and indicative of gestational diabetes if the fasting glucose level exceeds 105 mmol/L, or any 2 or 3 tests exceed 190, 165 and 145 mmol/L.
In the high-risk group, repeat the study of vaginal discharge for gonorrhea and PCR for. At 36 weeks of gestation, screening for group B streptococcus is carried out. In case of detection of streptococcus, a polymerase chain reaction (PCR) + treatment with intravenous penicillin preparations is performed before delivery.
Risk factors for preterm birth
- History of preterm birth
- Obstetric complications of pregnancy (twins, isthmic-cervical insufficiency, bleeding)
- Low body weight before pregnancy and inadequate weight gain during pregnancy
- Lower genital tract infections
- Adverse psychosocial factors
- vaginal bleeding
Threatening symptoms during pregnancy that require special attention
- Abdominal pain or cramps
- Frequent uterine contractions at 20-36 weeks
- Leakage of fluid from the vagina
- Significant reduction in fetal movements
- Severe headache or visual disturbances
- Constant nausea
- Fever or chills
- Swelling of the upper extremities or face
Common pregnancy complications that can be prevented or minimized with adequate prenatal care
- Iron and folate deficiency anemia
- Urinary tract infections, pyelonephritis
- during pregnancy (preeclampsia)
- preterm birth
- Retardation of intrauterine development of the fetus
- Sexually transmitted diseases and their impact on the newborn
- Rh immunization
- Fetal acrosomia
- Breech presentation of the fetus at term
- Hypoxia and fetal death due to delayed delivery