Why does a person have a wide pelvis. The pelvis as a whole. Age and sex differences, the size of the female pelvis
Page 3 of 6
TAZ IN GENERAL
Pelvis(pelvis) is formed by the connecting pelvic bones and the sacrum. It is a bone ring (Fig. 111). The pelvis is home to many internal organs. With the help of the pelvic bones, the trunk is connected with the lower extremities. There are two sections - a large and a small pelvis.
Big pelvis(pelvis major) is delimited from the lower pelvis by a border line. Border line(linea terminаlis) passes through the promontory of the sacrum, along the arcuate lines of the iliac bones, the crests of the pubic bones and the upper edge of the pubic symphysis. The large pelvis is bounded behind by the body of the V lumbar vertebra, from the sides - by the wings of the ilium. In front of a large pelvis bone wall does not have.
Small pelvis(pelvis minor) behind it is limited by the pelvic surface of the sacrum and the ventral surface of the coccyx. The lateral walls of the pelvis are inner surface pelvic bones (below the borderline), sacrospinous and sacro-tuberous ligaments. The anterior wall of the small pelvis is the upper and lower branches of the pubic bones, the pubic symphysis.
The small basin has an inlet and outlet. Upper aperture (hole) of the pelvis(apertura pelvis superior) bounded by the border line. Exit from the pelvis - lower pelvic aperture(apertura pelvis inferior) behind it is limited by the coccyx, from the sides by sacro-tuberous ligaments, branches of the ischial bones, ischial tubercles, lower branches of the pubic bones, and in front by the pubic symphysis. The obturator opening located in the lateral walls of the small pelvis is closed by a fibrous obturator diaphragm(membrana obturatoria). Throwing over the obturator groove, the membrane limits obturator channel(canalis obturatorius). Vessels and a nerve pass through it from the pelvic cavity to the thigh. The side walls of the small pelvis also have a large and small sciatic foramen. Large sciatic foramen(forаmen ischiаdicum majus) is limited to the large sciatic notch and the sacrospinous ligament. Lesser sciatic foramen(forаmen ischiаdicum minus) is formed by a small sciatic notch, sacro-tuberous and sacrospinous ligaments.

Rice. 111. Male (A) and female (B) pelvis. The lines of the sizes of the large pelvis and the entrance to the small pelvis are indicated. 1 - distаntia cristаrum (distance between the iliac crests); 2 - transverse diameter; 3 - distаntia spinаrum (distance between the anterior superior iliac spines); 4 - true (gynecological) conjugate; 5 - oblique diameter.
The structure of the pelvis is associated with a person's gender. The upper aperture of the pelvis with the vertical position of the body in women forms an angle of 55-60 ° with the horizontal plane (Fig. 112). The pelvis in women is lower and wider, the sacrum is wider and shorter than in men. The promontory of the sacrum in women protrudes less forward. The ischial tubercles are more turned to the sides, the distance between them is greater than in men. The angle of convergence of the lower branches of the pubic bones in women is 90 ° (pubic arch), in men it is 70-75 ° (subpubic angle).
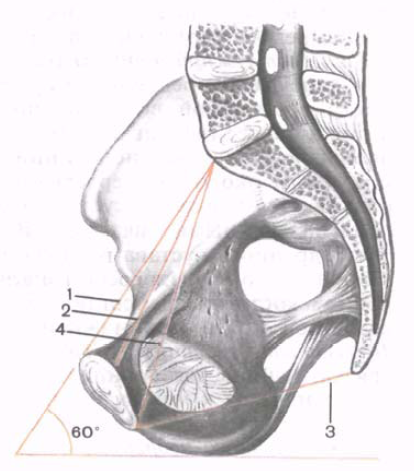
Rice. 112. Dimensions female pelvis... (Sagittal cut.) 1 - anatomical conjugate; 2 - true (gynecological) conjugate; 3 - straight size (exit from the pelvis); 4 - diagonal conjugate; 60 ° - the angle of inclination of the pelvis.
For forecasting generic process it is important to know the size of the woman's pelvis. The sizes of both the small and large pelvis are of practical importance. The distance between the two top and front iliac spines(distаntia spinаrum) in women is 25-27 cm.The distance between the most distant points of the wings iliac bones(distаntia cristаrum) is equal to 28-30 cm.
Direct size of the entrance to the small pelvis ( true, or gynecological, conjugate- conjugata vera, s. gynaecologica) is measured between the promontory of the sacrum and the most protruding posterior point of the pubic symphysis. This size is 11 cm.The transverse diameter (diameter transvérsa) of the entrance to the small pelvis - the distance between the most distant points of the boundary line - is 13 cm. Oblique diameter(diameter obliqua) of the entrance to the small pelvis is 12 cm. It is measured between the sacroiliac joint of one side of the pelvis and the ilio-pubic elevation of the other side.
The pelvis as a whole It is divided into large and small along the border through the sacral promontory (formed by the anterior part of the base of the sacrum and the body of the Y lumbar vertebra), through the arcuate lines of the ilium, the crests of the pubic bones and the upper edge of the pubic symphysis - the entire border is called the border line. The pelvic cavity is occupied internal organs and muscles, from below it is limited by the pelvic and urogenital diaphragms. The muscles of the lower girdle are located outside the pelvis.
V small pelvis distinguish between: the upper aperture (entrance), the cavity with wide and narrow parts, the lower aperture (exit). The upper aperture coincides with the border line, the lower one passes from behind through the apex of the coccyx, on the sides - through the sacro-tuberous ligaments, ischial tubercles, sciatic branches, in front - along the edge of the lower pubic branches and the lower edge of the pubic symphysis. On the front wall of the small pelvis there are obturator openings with the same canals, on the side walls there are large and small sciatic openings, bounded by the same bony notches and sacro-tuberous, sacrospinous ligaments.
Age differences in the structure of the pelvis are determined by changes in the angle of inclination and the degree of curvature of the sacrum and coccyx. Individual fluctuations in the angle of inclination of the pelvis (in men - in the range of 50-55 o, in women - 55-60 o) vary depending not only on gender, but also on the position of the body. In a sports or military stance, the angle of inclination increases as much as possible, in a sitting position it decreases as much as possible. Significant age-related fluctuations are also observed in terms of ossification of the pelvic ring bones.
Sex differences are manifested in the following:
• female pelvis, and especially its cavity, wide and low, with a cylindrical shape; male - narrow and tall with a conical cavity;
· The cape in women weakly protrudes into the cavity, forming an entrance in the form of an oval; the cape in men protrudes strongly, forming an entrance in the form of a card heart;
• the female sacrum is wide and short with a slightly concave, almost flat pelvic surface; male - narrow and long, strongly curved along the pelvic surface;
· Sub-pubic angle in women - more than 90 degrees, in men - 70-75 degrees;
· The wings of the iliac bones in women are more turned outward, and in men they have a more vertical position;
· The linear dimensions of the female pelvis prevail over those of men.
In the large pelvis in women, three transverse and one longitudinal size are distinguished:
· Interspinous size, as a direct distance of 23-25 cm between the anterior superior spines of the iliac bones;
· Inter-crestal size, as a straight distance of 26-28 cm between the most distant points of the iliac crests;
· Intertrochanteric dimension, as a direct distance of 30-33 cm between the most distant points of the greater trochanters;
· Longitudinal dimension, as a straight distance of 18-21 cm between the spinous process of the Y lumbar vertebra and the upper edge of the pubic symphysis.
All sizes of the large pelvis are measured with a thick compass in a living woman, since these bone formations are easily palpable. By the size of the large pelvis and its shape, one can indirectly judge the shape of the small pelvis.
In the small pelvis, there are transverse, oblique, longitudinal dimensions (diameters), which in each part of the pelvis (upper, lower apertures, cavity) are also measured between certain bony landmarks. So, for example, the transverse diameter of the entrance is the distance of 12-13 cm between the most spaced points of the arcuate line on the ilium; oblique diameter - 12 cm distance between the sacroiliac joint of one side and the ilio-pubic eminence opposite side; a straight size of 11 cm, as the distance between the cape and the point of the pubic symphysis most protruding posteriorly. The straight outlet size of 9 cm is the distance between the apex of the coccyx and the lower edge of the pubic symphysis; the transverse size of the outlet is 11 cm - the distance between the ischial tubercles. If you connect the midpoints of all straight dimensions, you get the wired axis of the small pelvis - a gentle curve, concavity facing the symphysis. This is the direction of movement of the child being born.
The hip joint is formed by the acetabulum of the pelvic bone and the head of the femur. To increase the articular surface along the edge of the acetabulum, there is a fibrous-cartilaginous acetabular lip with a transverse acetabular ligament. The articular capsule, consisting of fibrous and synovial membranes, is attached along the edge of the acetabular lip, and on femur along the neck: in front - along the intertrochanteric line, behind - inward from the intertrochanteric ridge. The capsule is strengthened by powerful ligaments: the circular zone, the ilio-femoral, pubic and sciatic-femoral ligaments. A ligament of the femoral head is located inside the joint, which during the period of its formation holds the head in the cavity.
The hip joint in shape refers to the spherical, triaxial, appearing as a kind of these joints - the cup-shaped joint. Around the frontal axis, flexion is performed in it with a bent knee at 118-121 o, with an unbent one - only at 84-87 o due to tension back muscles hips. Flexion is carried out by the muscles: iliopsoas, rectus femur, tailor's, comb, fascia lata tensor. They are supplied with blood by the following arteries: the ilio-lumbar, superior gluteal, obturator, external genital, deep and lateral surrounding the ilium, the descending knee, muscle branches of the femoral and deep femoral arteries. Innervation is carried out by the branches of the lumbar plexus, obturator, femoral and superior gluteal nerves
Knee-joint.
In education knee joint three bones are involved: the femur with the articular condylar surfaces, the patella with the posterior articular surface, the tibial with the upper articular surfaces on the medial and lateral condyles. Therefore, the joint is complex and condylar with insufficient correspondence of the articulating surfaces, which is complemented by fibro-cartilaginous menisci: medial and lateral. From this, the joint becomes complex.
The medial meniscus is narrow, lunar (in the form of the letter " WITH"); lateral meniscus - wide, oval (in the form of the letter " O"). In front, both menisci are connected by the transverse ligament of the knee, inside they grow to the intercondylar elevation of the tibia. A thin and loose capsule grows together with the outer edges of the menisci, its synovial membrane forms large pterygoid and numerous, small folds filled with adipose tissue, which increases the congruence of the articular surfaces. Paired pterygoid folds lie laterally and downward from the patella. The patellar fold - unpaired is located below the patella, located between it and the anterior intercondylar field.
The synovium in the joint forms pockets (sinuses, twists), the size and number of which is variable. Synovial bursae occur at the attachment points of muscle tendons: suprapatellar (the most extensive), subpatellar deep, hamstring pocket (behind - at the tendon of the muscle of the same name), bag of the sartorius muscle tendon, subcutaneous prepatellar bursa. Some bursae, connecting with the joint cavity, increase its volume.
The joint capsule is reinforced with internal and external ligaments. Internal ligaments include cruciate ligaments: anterior and posterior, filling the intercondylar fossa of the femur and the intercondylar field of the tibia. The extra-articular, external ligaments include: the collateral patellar and peroneal ligaments lying on the sides, the oblique popliteal and arcuate popliteal in the back, the patellar ligament (patellar) in the front, and the medial and lateral patellar support ligaments.
The knee joint is a typical condylar, complex and complex, in which the following movements are performed:
· Around the frontal axis: flexion and extension with a span of 140-150 about; flexion is inhibited by the cruciate ligaments and the quadriceps tendon; the condyles of the femur slide along the menisci;
· Around the longitudinal (vertical) axis, the volume of active rotation is on average 15 °, passive - 30-35 °; inward rotation is limited by cruciate ligaments, outward - by collateral ligaments.
The joints of the shin bones.
Tibia
The distal pineal gland has:
Fibula It has:
The shin bones have connections:
· tibiofibular joint formed by the flat articular surfaces of the peroneal head and upper epiphysis (lateral part), tibia; the articular capsule is taut and strengthened by the anterior and posterior ligaments of the fibular head; limited range of motion; sometimes the tibiofibular joint can communicate with the cavity of the knee joint;
· tibiofibular syndesmosis- a continuous connection by short and thick fibrous fibers between the peroneal notch on the distal epiphysis of the tibia and the articular surface of the lateral ankle, strengthened by the anterior and posterior tibiofibular ligaments, the synovial membrane of the ankle joint invades the tibiofibular syndesmosis;
· interosseous membrane of the lower leg- a fibrous membrane stretched between the interosseous edges of the greater and fibular bones in the area of their diaphysis; it has holes at the top and bottom for the passage of blood vessels and nerves.
In the joints of the lower leg bones, movements are almost absent, which is associated with support function the lower limb and the formation of a movable ankle joint.
· tibia
· fibula
· talus
Tibia on the proximal pineal gland has:
· Medial and lateral condyles with articular surfaces;
· Intercondylar eminence with medial and lateral tubercles :, anterior and posterior fields;
· The peroneal articular surface from the lateral side below the condyle.
On the diaphysis of the tibia are located:
· The anterior edge (acute) - upward passes into tuberosity, the lateral edge facing the fibula and the medial edge;
· Surfaces: medial, lateral and posterior with the soleus muscle line.
The distal pineal gland has:
· Peroneal notch along the lateral edge;
· The medial malleolus with the ankle groove at the back;
· Articular surfaces: ankle and lower.
The nuclei of ossification in the tibia appear in the proximal epiphysis at the end of the fetal period, in the distal - at the 2nd year of life, in the diaphysis - at the beginning of the fetal period. The final ossification occurs at the age of 19-24, the ankles at the age of 16-19.
Fibula It has:
· On the proximal epiphysis, the head, neck, on the head - the apex and articular surface;
On the diaphysis: anterior, posterior and interosseous edges; lateral, posterior and medial surfaces;
· On the distal epiphysis: the lateral malleolus with the articular surface and the fossa (behind).
Secondary nuclei of ossification appear in the distal pineal gland at the 2nd year of life, in the proximal at 3-5 years, the final ossification at 20-24 years.
Ankle joint.
The formation of the joint involves:
· The tibia with its lower and medial malleolar articular surfaces;
· The fibula with the articular surface of the lateral malleolus;
· Talus of the upper and ankle (medial and lateral) articular surfaces located on the block;
· The ankles are forking around the block, forming a typical block joint - complex due to the articulation of three bones.
The articular capsule is attached from the back along the edge of the articular surfaces of the bones that make up the joint, in front by 0.5-1 cm above it.
On the sides, the capsule is thick and strong, in front and behind it is thin, loose, folded; reinforced by lateral ligaments:
· medial(deltoid) - thick, strong, fanning out from the medial malleolus to the talus, scaphoid and calcaneus; in the ligament, parts are distinguished: tibial-navicular, tibial-calcaneal, anterior and posterior tibial-talus;
· lateral as part of the anterior talofibular, posterior talofibular, calcaneofibular ligaments.
The ligaments are so strong, especially the medial, that, with maximum stretching, they can tear off the ankle.
In the ankle and talocalcaneonavicular joints, the following movements are performed:
· flexion(plantar) and extension (sometimes called dorsiflexion) around the frontal axis with a span of 60 degrees;
· adduction and abduction around the sagittal axis with a span of 17 degrees;
· pronation and supination around the vertical axis with a span of 22 degrees.
The joint of the foot.
Foot bones subdivided into tarsal bones: 7 short cancellous bones and bones of the metatarsus consisting of 5 short tubular bones; and also phalanges of the fingers - three in each finger, except for the first, which has two phalanges. The bones of the tarsus lie in two rows: in the proximal (posterior) - the talus and calcaneal, in the distal (anterior) - scaphoid, wedge-shaped: medial, intermediate, lateral and cuboid bones.
Talus consists of a body, head, neck. On top of the body there is a block with the superior, medial and lateral ankle articular surfaces. Below on the body are the heel articular surfaces: anterior, middle and posterior. Between the middle and posterior calcaneal surfaces is the talus groove. The scaphoid articular surface lies on the head. The talus has processes: lateral and posterior, on the latter - the medial and lateral tubercles, separated by a groove for the tendon of the long flexor of the thumb.
Heel bone has a body, ending posteriorly with a calcaneal tubercle. On the body, the talus articular surfaces are distinguished: anterior, middle and posterior. Between the middle and the posterior is the groove of the calcaneus, which, together with the groove of the talus, forms the tarsal sinus. At the distal end of the body there is a cuboid articular surface. The processes and other grooves of the calcaneus are the supporting process of the talus on the medial surface, the groove of the tendon of the long peroneal muscle on the lateral surface.
Scaphoid at the distal end it has three articular surfaces for the sphenoid bones, tuberosity along the medial edge for attaching the posterior tibial muscle.
Sphenoid bones have a characteristic triangular shape, and on the front and back sides and on the sides - articular surfaces - in front for articulation with the first three metatarsal bones, behind for connection with the scaphoid bone, on the sides for articulation with each other and the cuboid bone.
Cuboid also has articular surfaces in the back for articulation with the calcaneus, in front - with the metacarpal bones, and along the medial surface - for connecting the lateral sphenoid and scaphoid bones. On the lower surface there is a tuberosity and a groove for the tendon of the peroneus longus muscle.
Metatarsal bones and phalanges- These are short tubular bones, each of which consists of a base, body and head. The articular surfaces are at the head and base. The head of the first metatarsal bone from below is divided into two platforms, with which the sesamoid bones are in contact. On the lateral surface of the Y metatarsal bone there is a tuberosity for the attachment of the short peroneal muscle. Each distal (nail) phalanx ends with a tubercle for the attachment of muscle tendons.
The primary nuclei of ossification appear in the calcaneus at the 6th month of the fetal period, in the talus at 7-8, in the cuboid at the 9th month. In the remaining bones of the tarsus, secondary nuclei are formed: in the lateral wedge-shaped - at the 1st year, in the medial wedge-shaped - by 3-4, in the scaphoid - at 4-5 years, complete ossification - at 12-16 years.
The metatarsal bones begin to ossify in the epiphyses at 3-6 years old, complete ossification - at 12-16 years old. The diaphysis of the phalanges and metatarsal bones form the primary nuclei at 12-14 weeks of the fetal period, the secondary ones in the phalanges at 3-4 years, complete ossification of the phalanges at 18-20 years
The following are involved in the formation of the ankle joint:
· tibia its lower and medial ankle articular surfaces;
· fibula- the articular surface of the lateral ankle;
· talus- upper and ankle (medial and lateral articular surfaces) located on the block.
The ankles are forked around the block, forming a typical blocky joint, complex due to the articulation of three bones.
The articular capsule is attached from the back along the edge of the articular surfaces of the articulating bones, in front by 0.5-1 cm above it.
On the sides, the capsule is thick and strong, in front and behind it is thin, loose, folded, reinforced with powerful lateral ligaments:
· Medial (deltoid) - thick, strong, fanning out from the medial malleolus to the talus, scaphoid and calcaneus; in the ligament, parts are distinguished: tibial-navicular, tibial-calcaneal, anterior and posterior tibial-talus;
· Lateral as part of the anterior talofibular, posterior talofibular, calcaneofibular ligaments.
The ligaments are so strong, especially the medial, that, with maximum stretching, they can tear off the ankle.
The following movements are performed in the ankle joint:
· flexion(plantar) and extension (dorsiflexion) around the frontal axis with a span of 60 about;
· adduction and abduction around the sagittal axis with a span of 17 about;
· pronation and supination around the vertical axis with a span of 22 about.
Subtalar joint formed by the posterior articular surfaces of the talus and calcaneus, which match well. The capsule at the joint is thin, stretched, reinforced with ankle ligaments.
Talocalcaneonavicular joint formed by the articular surface on the head of the talus, which articulates in front with the scaphoid bone, and below with the calcaneus. The articular surface of the calcaneus is complemented by the plantar calcaneonavicular ligament, which at the head of the talus passes into fibrous cartilage. The articular capsule is attached along the edge of the articular surfaces, closing a single cavity. The capsule is strengthened by strong ligaments: the interosseous talocalcaneal up to 0.5 cm thick and from above - the talo-navicular. When stretching them (especially the talocalcaneal ligament), the head of the talus is lowered and the foot is flattened.
The joint is spherical in shape, but with one sagittal axis of motion. Together with the subtalar joint, it forms a combined joint with a limited range of motion in the form of adduction and abduction, turning the foot outward and inward. The total volume of all movements does not exceed 55 o. In a newborn and infant this joint is in a supinated position, with the beginning of walking, pronation gradually occurs with the lowering of the medial edge of the foot.
Heel-cuboid joint- saddle with great congruence of articular surfaces; the joint capsule is thick and taut on the medial side, thin and loose on the lateral side, reinforced with ligaments: plantar calcaneal-cuboid and long plantar. Movements in a limited amount are carried out around the longitudinal axis in the form of a slight rotation, complementing the movements in the talocalcaneonavicular joint.
The transverse (Choparov) joint of the tarsus includes the calcaneo-cuboid and talo-navicular joints so that the joint space takes the form of the Latin S, passing across the foot. Common ligament of joints - bifurcated ( lig. bifurcatum) - serves as a kind of key, when dissected, the joint cavity opens wide. It has a Y-shaped appearance and consists of the calcaneonavicular and calcaneo-cuboid ligaments.
Wedge-navicular joint- flat, complex, as it is formed by three wedge-shaped and one navicular bones, reinforced by the dorsal and plantar wedge-navicular and intra-articular intercliniform ligaments. The joint cavity can communicate with the tarsometatarsal joints.
Tarsometatarsal (Lisfranc) joints- flat with limited range of motion, include the following three joints:
· The joint between the medial sphenoid and first metatarsal bones;
· The joint between the intermediate, lateral sphenoid bones and II, III metatarsal;
· The joint between the cuboid bone and the IY, Y metatarsal bones;
· The tarsometatarsal joints are strengthened by the tarso-metatarsal ligaments (dorsal and plantar) and interosseous cuneiform ligaments, of which the medial cuneiform ligament is considered in practice to be the key of these joints.
Intermetatarsal joints- flat, formed by the lateral surfaces of the bases of the metatarsal bones, reinforced by the dorsal and plantar metatarsal interosseous ligaments. Movement in them is severely limited.
Metatarsophalangeal joints formed by the spherical heads of the metatarsal bones and the concave bases of the proximal phalanges. The capsules are thin, loose, reinforced with collateral and plantar ligaments. The deep transverse metatarsal ligament connects the metatarsal heads and strengthens the joint capsules. Flexion and extension in them is 90 o, adduction and abduction are limited.
Interphalangeal joints- proximal and distal, except for the thumb joint, where there is one interphalangeal joint. They belong to blocky joints, strengthened by collateral and plantar ligaments.
The human foot has lost the adaptations of the grasping organ, but has acquired the arches necessary for support and movement of the whole body.
The bones of the tarsus and metatarsal are connected by sedentary joints.
Moreover, due to the shape of the bones and their "tight" joints, five longitudinal and one transverse vaults were formed upwardly convex with points of support on the calcaneal tubercle and the heads of the I and Y metatarsal bones.
The longitudinal vaults run along the long axis of the metatarsal bones: from their heads, through the body to the base and further through the adjacent tarsal bones to the calcaneal tuberosity, where they all converge. The longest and highest is the second vault.
The medial longitudinal vaults perform the spring (springing) function, the lateral ones - the supporting one. At the level of the most high points the longitudinal vaults are transverse.
The vaults are held in place due to the shape of bones and joints, reinforced with passive "puffs" - ligaments with the plantar aponeurosis and active "puffs" - muscles and their tendons. The longitudinal arches strengthen the following ligaments: long plantar, calcaneonavicular and plantar aponeurosis. The transverse arch is held by the metatarsal transverse and interosseous ligaments. The tendons of the long flexors and extensors of the fingers, the tibial muscles, as well as the short flexors of the fingers, the vermiform muscles strengthen the longitudinal arches. The transverse arch is held by the square sole of the sole, adductor and interosseous muscles.
In the process of human evolution, major changes have occurred in the foot, associated with its vaulted structure. Three support points were formed on the sole - the heel and the bases of the first and fifth toes, the tarsal bones increased in size, and the phalanges of the toes were significantly shortened. The joints of the foot became stiff. Attachment of the long muscles of the leg and short muscles of the foot has shifted medially towards thumb, which strengthens the pronation of the foot and strengthens the arches. The loss of acquired properties is accompanied by the development of flat feet, which is a disease for humans.
The pelvic bones, sacrum, tailbone and their ligaments form the pelvis (pelvis). Its upper section is a large pelvis (pelvis major) wide, is part abdominal cavity, from the sides it is limited by the wings of the iliac bones, from the back - by the V lumbar vertebra and the lumbar-iliac ligament, the anterior wall is formed by muscles (Fig. 37). Downward, the large pelvis passes into the small pelvis (pelvis minor). The plane separating them, called the upper aperture of the small pelvis, is limited by the protrusion of the sacrum, the arcuate line of the ilium, the crest of the pubic bone and the upper edge of the pubic symphysis. The walls of the small pelvis are: in front - symphysis, behind - sacrum and coccyx, from sides - pelvic bones and their bundles. The lower aperture of the small pelvis, or its outlet, is limited by the coccyx, the sacro-tubercular ligament, the sciatic tubercle, the branches of the sciatic and pubic bones and the lower edge of the symphysis.
Like other bone cavities, the pelvis protects the internal organs in it (rectum, bladder, in women - the ovaries, fallopian tubes, uterus, vagina, and in men - the prostate gland and seminal vesicles). The mechanical significance of the bone ring of the pelvis is great. The severity of the head and trunk is transmitted through the sacrum and pelvic bones to lower limbs... In this case, the sacrum and pelvic bones act as a solid vault. In addition to this, the bone pelvis is directly related to one of the most important functions of the body - childbirth. Therefore, there are significant differences in the structure of the pelvis of men and women.
Sex differences in the structure of the pelvis (Fig. 38; see Fig. 37). The female pelvis is lower and wider, and the male pelvis is higher and narrower. The wings of the ilium in women are turned to the sides, and in men they are more vertical. In men, the pelvic cavity narrows downward. In the area of the upper aperture, the promontory of the sacrum sharply protrudes forward, the cavity of the small pelvis narrows by closely located ischial spines and tubercles, the symphysis is narrow, high, the exit from the small pelvis is also limited by the protruding coccyx. In general, the pelvic cavity in men seems to be compressed from the sides. In the female pelvis, on the contrary, the entrance to the small pelvis looks like a smooth transverse oval, the promontory of the sacrum does not protrude, the sciatic tubercles are further apart, the symphysis is low, wide, the sacrum is flat, the tailbone protrudes not sharply into the lumen of the exit from the small pelvis. In general, the pelvis looks like a wide cylinder. The lower branches of the pubic bones in women form a wide arc, and in men - an acute angle. During pregnancy, the fibrous cartilage of the interpubic disc loosens, the cartilage itself and the cavity in it increase, the symphysis becomes wider, which further increases the internal cavity of the small pelvis. Many bony points of the pelvis can be felt on a living person (iliac crests, upper anterior iliac spines, symphysis, ischial tubercles, etc.). This makes it possible to obtain important obstetric practice the size of the large and small pelvis. They are determined with a special obstetric compass-pelvimeter.
The size of the large pelvis of a woman (Fig. 39). The spinous distance (distantia spinarum) is 25 - 27 cm. To determine it, the legs of the compass are placed on the upper anterior spines of the ilium.
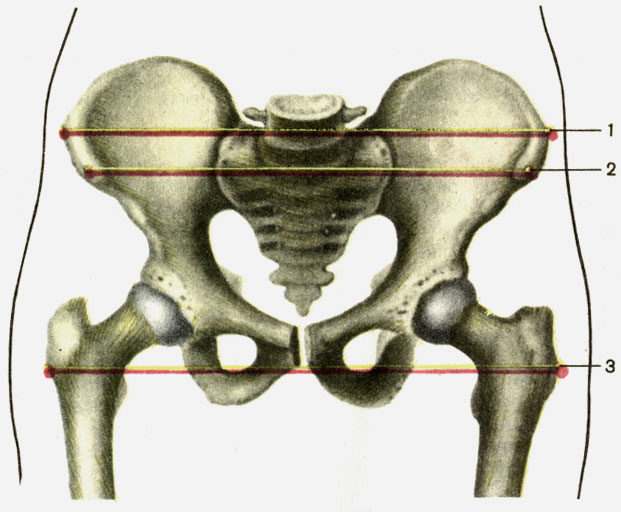
The crestal distance (distantia cristarum) is 28 - 29 cm. The legs of the compass are located at the most distant points of the iliac crests.
Trochanteric distance (distantia trochanterica) is 30 - 32 cm. This is the distance between the greater trochanters of the femur.
The size of the small pelvis of a woman (Fig. 40). The anteroposterior dimensions in the pelvic area of a woman are called straight dimensions or conjugates.
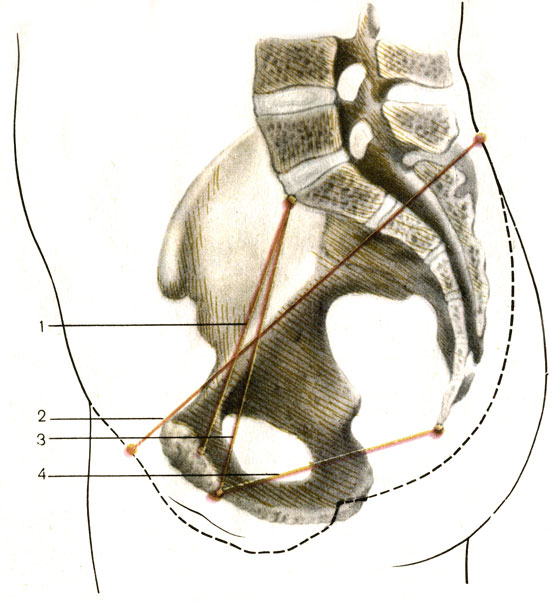
The external conjugate, or external straight size, is 21 cm. To determine it, one leg of the compass is placed on the skin in the region of the upper edge of the pubic symphysis, and the other on the skin in the fossa between the last lumbar and I sacral vertebra.
A very important true, or obstetric, conjugata vera. It characterizes the smallest direct size of the entrance to the small pelvis: between the promontory of the sacrum and the point of the pubic symphysis most protruding posteriorly. On average, the true conjugate is 10.5 - 11.0 cm. It can be determined in two ways. The first method consists in subtracting 10 cm from the value of the external straight size (21 cm). The second method involves a vaginal examination. In this case, the distance between the promontory of the sacrum and the lower edge of the pubic symphysis is determined. From the resulting figure (12.5 - 13.0 cm), subtract 2 cm.
The direct size of the exit from the small pelvis is on average 10 cm.
To determine it, one leg of the compass is placed on the skin in the coccyx region, and the other on the lower edge of the symphysis. Subtract 2 cm from the resulting figure (12 cm).
The transverse size of the entrance is 13.5 - 15.0 cm. It is found indirectly: the value of the ridge distance is divided in half.
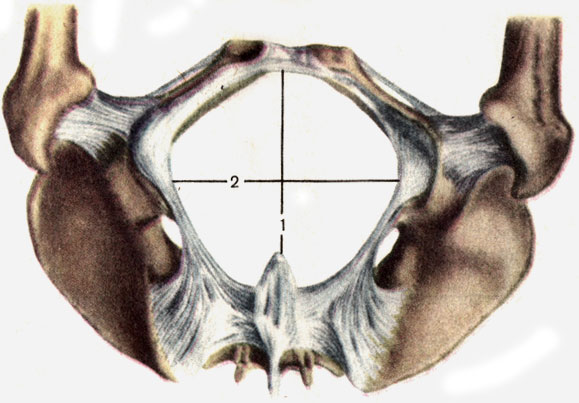
The transverse size of the exit from the small pelvis is 11 cm (see Fig. 38). The legs of the compass are placed on the inner edges of the ischial tubercles. To the resulting figure (9 - 10 cm) add 1.0 - 1.5 cm (correction for the thickness of soft tissues).