Upper posterior iliac spine in Latin. Lower limb bones and their joints
The famous British neurophysiologist Chris Frith is well known for his ability to speak simply about very complex problems of psychology - such as mental activity, social behavior, autism and schizophrenia. It is in this area, along with the study of how we perceive the world, we act, make a choice, remember and feel, today there is a scientific revolution associated with the introduction of neuroimaging methods. In the book "Brain and Soul" Chris Frith talks about all this in the most accessible and entertaining way.
440 rub
Human anatomy. Atlas coloring
The bestseller Human Anatomy: Coloring Atlas has been the leader among educational atlases for over 35 years. This is a unique guide: its concise text and accurate hand-drawn illustrations are specially designed for interactive learning of anatomy - coloring.
The original color key, visual associations and interactive learning are easier, more interesting and more effective. A verified visual structure, easy navigation and short explanatory texts will allow students medical universities learn anatomy quickly and reliably. Wide circle readers will be able to connect ideas about different systems and organs into a single whole and understand human anatomy on an equal basis with professionals.
949 rub
human anatomy
The Atlas of Human Anatomy: 2nd Edition is compact and easy to use for students of all medical specialties. It will serve as a reliable and easy reference for health conscious people. It contains 200 color drawings with designations and comments to them: the structure of the body is given in classical sequence starting with the living cell and the musculoskeletal system and ending with the senses. Internal organs (digestive, respiratory system, genitourinary apparatus), the cardiovascular system, hematopoietic organs and the immune system, endocrine glands, nervous system- clearly presented taking into account the results of new scientific research.
389 rub
Body guide. A practical guide to body palpation
The Body Guide is a unique guide to palpation of the musculoskeletal system. In the structure of this book, body areas and movements in the body are considered according to the logic of their interaction: shoulder girdle and shoulder, forearm and hand, spine and trunk, head, neck and face, pelvis and thigh, lower leg and foot. Each area is detailed, from superficial anatomy, skin and fascia, to muscle and bone.
In total, the book describes 162 muscles, 206 bones, 33 ligaments and 110 bony landmarks. The total number of illustrations is about 1400. The Appendix provides valuable information on synergistic muscles, facial muscles and a reference to trigger points.
For chiropractors, osteopaths, massage specialists, physiotherapists, physiotherapy specialists.
3429 rub
Biophysics of the senses
The book describes the biophysical foundations and mechanisms of the functioning of the sense organs of not only humans, but also animals.
It draws parallels between the functioning of different senses, provides evidence that all senses are built on the basis of the same receptor. After reading the book, you will learn:
that all our senses are created by nature on the basis of one sensitive element; what parameter of a molecule determines its smell;
how do electrical impulses in our senses;
why our senses are equipped with a logarithmic scale;
how the vestibular apparatus works;
how live radars work;
how the bird's compass works;
what are fishy feelings.
The book is designed for high school students, students and anyone interested in popular physiology.
340 rub
Nutrition, microbiocenosis and human intelligence
The book extensively discusses the problems associated with issues of clinical nutrition. Submitted by new system views on the nature of diseases internal organs person taking into account of particular importance endo-ecological system (microbiota). Some new principles of clinical nutrition are presented, including using biotechnological approaches aimed at controlling physiological functions through the use of artificial nutrition or microbiota correction. The current achievements and prospects for the use of nutritional therapy for a number of diseases are highlighted: "nutritional-metabolic therapy", "functional nutrition", microbiota correction, and so on. For the first time, opportunities for increasing intellectual abilities a person using nutritional approaches through the prism of a new paradigm of neuropsychonutriciology.
The manual is intended for physiologists, psychologists, microbiologists, therapists, gastroenterologists, surgeons, clinical pharmacologists, nutritionists, general practitioners, medical students - anyone who is constantly striving to expand the boundaries of their knowledge about the essence of the material world.
159 rub
Atlas of Human Anatomy (set of 3 books)
Human Anatomy Atlas - Important tutorial for medical students, as well as for anyone studying medicine, biology, psychology and other human sciences. An anatomical atlas can be a useful book in any family library.
Atlas is written with modern achievements medical science, it reflects the established traditions and sequence of studying the human body, its organs, systems and apparatuses.
In the Atlas, along with drawings traditionally showing appearance various bodies, there are pictures of the macro-micro- and microscopic structure of organs and tissues, as well as accompanying figures, text, diagrams and tables that help to better understand and evaluate the structure and structure of the organs of the human body.
8090 rub
Sphincterology
Sphincterology is the study of the structural and functional organization of sphincters, of the locking apparatus and valve devices of various human organs and systems.
The monograph presents the latest scientific data on the mechanisms of regulation of the locking devices of various organs, their design at the stages of ontogenesis. Outlined modern views about the structure and function of the human sphincter apparatus. The data on the vascular and nervous devices of these organs, and in some cases on their age and individual characteristics... A very bright and varied morphological picture of valve structures is described in detail. digestive tract... The issues of the functioning of the compression devices of the biliary system and the genitourinary apparatus are highlighted in sufficient detail.
Considerable attention is paid to the issues of localization, form, presence of antagonists, frequency of occurrence and additional components locking mechanisms of the human body. Submitted by modern classification and complete list loopback structures of human organs and systems.
The monograph is intended for morphologists, therapists, gastroenterologists, surgeons, urologists, radiologists, endoscopists.
...165 rub
This two-volume richly illustrated work on human anatomy is the first English translation of the Soviet textbook by M. Prives, N. Lysenkov, and V. Bushkovich. Unique in its analytic and synthetic approaches to the subject, the book covers descriptive, evolutionary, functional and practical anatomy. The human organism is studied in depth as the product of long and continuing evolution, and both traditional anatomy and new directions in anatomical science are treated fully. The clear and detailed discussions of the influence of sports and various occupations on the human body will be of particular interest.
Volume I covers the following subjects: the history of anatomy, the science of bones and their articulations, myology, the science of viscera, and the science of the organs of internal secretion.
Volume II deals with the anatomy about the heart and blood-vascular system the lymphatic system, the organs оf haemopoiesis and immunological reactions, the nervous system and the sense organs. The phylogenesis and ontogenesis of the organs are discussed in detail. The effect of social factors on the structure of the organism is described. The importance of the principle of integrity in anatomy is stressed, namely that anatomy is a science of the structure not only of the separate systems but of the whole organism human organism. The description of the structure of the human body is supplemented by synthesis of the anatomical data as a result about which the human organism is represented as an integrity, a complex system of interrelationship of components and processes. The textbook is intended for anatomists and university students.
3809 rub
The skeleton of the lower extremities (Fig. 44) is divided into two sections: the skeleton of the girdle of the lower extremities ( pelvic girdle, or pelvis) and the skeleton of the free lower limbs.
Lower limb girdle bones
The skeleton of the girdle of the lower extremities is formed by two pelvic bones and a sacrum with a coccyx.
Hip bone(os coxae) in children consists of three bones: the iliac, pubic and sciatic, connected in the acetabulum by cartilage. After 16 years, the cartilage is replaced by bone tissue and a monolithic pelvic bone is formed (Fig. 45).
Ilium(os ilium) - the largest part pelvic bone, makes up its upper section. In it, a thickened part is distinguished - the body and a flat section - the wing of the ilium, ending in a ridge. On the wing in front and behind there are two protrusions: in front - the upper anterior and lower anterior iliac spines, and behind - the upper posterior and lower posterior iliac spines. The superior anterior iliac spine is well palpable. On inner surface the wing has an iliac fossa, and on the gluteal (outer) - three rough gluteal lines - anterior, posterior and lower. The gluteal muscles begin from these lines. Rear part the wing is thickened, on it there is an ear-shaped (articular) surface for articulation with the sacrum.
Pubic bone(os pubis) is the front of the pelvic bone. It consists of a body and two branches: upper and lower. On the upper branch of the pubic bone is the pubic tubercle and the pubic ridge, which passes into the arcuate line of the ilium. At the junction of the pubic bone with the ilium, there is an ilio-pubic elevation.
Ischium(os ischii) forms lower part the pelvic bone. It consists of a body and a branch. The lower part of the branch of the bone has a thickening - the sciatic tubercle. At the posterior edge of the body of the bone there is a protrusion - the ischial spine, separating the greater and lesser ischial notches.
The branches of the pubic and ischial bones form the obturator opening. It is closed by a thin connective tissue obturator membrane. In its upper part there is an obturator canal, limited by the obturator groove of the pubic bone. The channel serves for the passage of the vessels of the same name and the nerve. On the outer surface of the pelvic bone, at the junction of the bodies of the ilium, pubic and ischial bones, a significant depression is formed - the acetabulum,
The pelvis as a whole
The pelvis (pelvis) is formed by two pelvic bones, the sacrum and the coccyx.
Pelvic bone joints... The pelvic bones are connected in front by the pubic symphysis, and behind - by two sacroiliac joints (Fig. 46) and numerous ligaments.
Pubic symphysis formed by the pubic bones, tightly fused with the fibro-cartilaginous interpubic disc located between them. There is a slit cavity inside the disc. This symphysis is strengthened by special ligaments: from above - by the superior pubic ligament and from below - by the arcuate ligament of the pubis. During pregnancy, the cavity of the pubic symphysis increases. A slight expansion of the sacroiliac joint cavity is also possible. Due to the expansion of these cavities, the size of the pelvis increases, which is a favorable factor during childbirth.
Sacroiliac joint flat in shape, formed by the ear-shaped surfaces of the sacrum and the ilium. Movement in it is extremely limited, which is facilitated by a system of powerful ventral (anterior), dorsal (posterior) and interosseous sacroiliac ligaments.
TO pelvic ligaments include the sacro-tuberous ligament - goes from the sacrum to the sciatic tubercle and the sacrospinous ligament - goes from the sacrum to the sciatic spine. These ligaments close the greater and lesser sciatic notches, forming together with them the greater and lesser sciatic foramen, through which muscles, blood vessels and nerves pass. The posterior part of the iliac crest is connected to the transverse process of the V lumbar vertebra by a strong ilio-lumbar ligament.
Large and small pelvis... The border line, which runs along the upper edge of the pubic symphysis, the crests of the pubic bones, the semicircular lines of the ilium and the promontory of the sacrum, the pelvis is divided into two sections: the large and small pelvis.
The large pelvis is bounded by the wings of the ilium, the small one - by the ischial and pubic bones, sacrum, coccyx, sacro-tuberous and sacrospinous ligaments, obturator membranes and pubic symphysis. There are two holes in the pelvic cavity: the upper one is the upper aperture of the pelvis (inlet) and the lower one is the lower aperture of the pelvis (outlet). The upper aperture is limited by the boundary line, and the lower - by the branches of the pubic and ischial bones, ischial tubercles, sacro-tuberous ligaments and the coccyx.
Sex differences in the pelvis... The shape and size of the female pelvis differs from the male (Fig. 47). The female pelvis is wider and shorter in height than the male. His bones are thinner, their relief is smoothed. This is due to differences in the degree of muscle development between women and men. The wings of the male pelvis are located almost vertically; in women, they are turned to the sides. The volume of the small pelvis in women is greater than that of men. Cavity female pelvis is a cylindrical channel, in men it resembles a funnel.
The subpubic angle, formed by the lower branches of the pubic bones (its apex is located at the lower edge of the pubic symphysis), also has sex differences. In men, this angle is acute (about 75 °), and in women it is obtuse and has the shape of an arc (sub-pubic arch).
The upper aperture of the pelvis in women is wider than in men and has an elliptical shape. In men, she heart-shaped due to the fact that their cape protrudes more forward. The lower pelvic aperture is also wider in women than in men. Sexual differences in the pelvis begin to emerge at the age of over 10 years.
Anatomical data on the structural features and dimensions of a woman's pelvis are taken into account in obstetrics. It is customary to define following sizes large and small pelvis (Fig. 48, 49).
The average size of the large pelvis in a woman: 1) spinous distance (distantia spinarum), that is, the distance between the anterior superior spines of the iliac bones, is equal to 25 - 27 cm;
2) the ridge distance (distantia cristarum), that is, the distance between the points of the iliac crests most distant from each other, is 28 - 29 cm;
3) trochanteric distance (distantia trochanterica), that is, the distance between the greater trochanters of the femur, is 30 - 32 cm;
4) the external straight size, that is, the distance between the upper edge of the pubic symphysis and the depression between the spinous process of the V lumbar vertebra and the sacrum, is 21 cm.
Bone landmarks for determining the indicated dimensions are found by palpation, and the distance between them is measured using a special compass - a pelvis meter.
The average size of the small pelvis in a woman: 1) anatomical conjugate, or straight diameter (diametr recta), that is, the distance between the cape and the upper edge of the pubic symphysis, 11 cm.
2) the transverse diameter (diametr transversa), that is, the distance between the points of the boundary line most distant from each other, located in the frontal plane, is 13 cm;
3) obstetric, or true, conjugate (canjugata vera), that is, the distance between the cape and the back point of the symphysis that protrudes most into the pelvic cavity, is on average 10.5 cm and characterizes the smallest anteroposterior size of the pelvic cavity. The true conjugate is determined indirectly by the external direct size of the pelvis (10 cm is subtracted from it) or by the diagonal conjugate. The diagonal conjugate is the distance between the promontory and the lower edge of the symphysis (about 12.5 cm). The true conjugate is less than the diagonal by an average of 2 cm. The diagonal conjugate is determined by vaginal examination;
4) the straight diameter of the exit from the small pelvis, that is, the distance from the lower edge of the symphysis to the apex of the coccyx, is 10 cm. During childbirth, it increases to 15 cm due to the deviation of the coccyx back;
5) the transverse size of the exit of the small pelvis, that is, the distance between the tubercles of the ischial bones, is 11 cm.
The imaginary line connecting the mid-anteroposterior dimensions of the entrance to the small pelvis, the cavity of the small pelvis and the exit from the small pelvis is the axis of the pelvis. It is also called a wire axis or guide line; it is the path that the fetal head travels during labor. The axis of the pelvis is a curved line, its curvature approximately corresponds to the curvature of the pelvic surface of the sacrum.
The pelvis is tilted anteriorly (when the body is upright). The angle of inclination of the pelvis is formed by a line drawn through the promontory and top edge the pubic symphysis, and the horizontal plane. Usually it is 50 - 60 °.
Bones of the free lower limb
Skeleton free lower limbs(legs) includes the femur with the patella, the bones of the lower leg and the bones of the foot (see Fig. 44).
Femur(femur) - the most long bone the human body (Fig. 50). It distinguishes between the body, proximal and distal ends. The ball-shaped head at the proximal end faces the medial side. Below the head is the neck; it is located at an obtuse angle to the longitudinal axis of the bone. At the place of transition of the neck into the body of the bone, there are two protrusions: a large trochanter and a small trochanter (trochanter major and trochanter minor). The large spit lies outside and is easy to feel. An intertrochanteric crest runs between the trochanters on the posterior surface of the bone, and the intertrochanteric line runs along the anterior surface.
Body femur curved, the bulge is directed anteriorly. The anterior surface of the body is smooth; a rough line runs along the posterior surface. The distal end of the bone is somewhat flattened from front to back and ends in lateral and medial condyles. Above them from the sides, the medial and lateral epicondyle rises, respectively. Between the latter, the intercondylar fossa is located behind, and the patellar surface in front (for articulation with the patella). Above the intercondylar fossa there is a flat, triangular popliteal surface. The condyles of the femur have articular surfaces to connect to the tibia.
Patella(patella), or patella, is the largest sesamoid bone; it is enclosed in the tendon of the quadriceps femoris muscle and is involved in the formation of the knee joint. On it, an expanded upper part is distinguished - the base and a narrowed, downward-facing part - the top.
Shin bones: tibial, located medially, and peroneal, takes a lateral position (Fig. 51).
Tibia(tibia) consists of a body and two ends. The proximal end is much thicker; it has two condyles: medial and lateral, articulating with the condyles of the femur. The intercondylar eminence is located between the condyles. On outside the lateral condyle is a small peroneal articular surface (for connection with the head of the fibula).
The body of the tibia is triangular in shape. The anterior edge of the bone protrudes sharply, at the top it passes into a tuberosity. At the lower end of the bone from the medial side, there is a downward process - the medial malleolus. Below, at the distal end of the bone, there is an articular surface for combination with the talus, on the lateral side there is a peroneal notch (for connection with the fibula).
Fibula(fibula) - relatively thin, located outward from the tibia. The upper end of the fibula is thickened and called the head. On the head, an apex is distinguished, facing outward and backward. The fibular head articulates with the tibia. The body of the bone has a triangular shape. The lower end of the bone is thickened, is called the lateral malleolus and is adjacent to the talus from the outside. The edges of the shin bones facing each other are called interosseous; the interosseous membrane (membrane) of the lower leg is attached to them.
Foot bones divided into the bones of the tarsus, metatarsal bones and phalanges (fingers) (Fig. 52).
Tarsal bones belong to short spongy bones. There are seven of them: ram, calcaneal, cuboid, scaphoid and three wedge-shaped. The talus has a body and a head. On top surface her body is a block; together with the bones of the lower leg, it forms the ankle joint. Under the talus is the calcaneus, the largest of the tarsal bones. On this bone, a well-pronounced thickening is distinguished - the tubercle of the calcaneus, a process called the support of the talus, the talus and cuboid articular surfaces will serve to connect with the corresponding bones).
In front of the calcaneus is the cuboid bone, and anterior to the head of the talus lies the scaphoid. Three sphenoid bones - medial, intermediate and lateral - are located distal to the scaphoid bone.
Metatarsal bones in the amount of five are located anterior to the cuboid and sphenoid bones. Each metatarsal bone consists of a base, body, and head. With their bases, they articulate with the bones of the tarsus, and with their heads - with the proximal phalanges of the fingers.
The toes, like the fingers, have three phalanges, except for the first finger, which has two phalanges.
The skeleton of the foot has features due to its role as a part support apparatus with an upright body position. The longitudinal axis of the foot is almost at right angles to the axis of the lower leg and thigh. In this case, the bones of the foot do not lie in the same plane, but form transverse and longitudinal arches, facing the concavity towards the sole, and the convexity towards the rear of the foot. Due to this, the foot is supported only by the tubercle of the calcaneus and the heads of the metatarsal bones. The outer edge of the foot is lower, it almost touches the surface of the support and is called the support arch. The inner edge of the foot is raised - this is a spring arch. Such a structure of the foot ensures that it performs its supporting and spring functions, which is associated with the vertical position of the human body and upright posture.
Connections of the bones of the free lower limb
Hip joint(articulatio coxae) is formed by the acetabulum of the pelvic bone and the head of the femur. The acetabular (articular) lip is located along the edge of the acetabulum, making the cavity deeper. In shape, this is a type of ball joint - a nut joint.
The joint is reinforced with ligaments. The strongest ilio-femoral ligament. It goes obliquely in front of the joint from the anterior lower iliac spine to the intertrochanteric line of the femur and inhibits extension in hip joint... This bundle has great importance to keep the body upright. From the superior branch of the pubic bone and the body of the ischium, the pubic-femoral and ischio-femoral ligaments begin; they pass along the medial and posterior surfaces of the articular capsule, partly woven into it, and are attached to the lesser and greater trochanters of the femur.
Inside the joint cavity is the ligament of the femoral head. It runs from the bottom of the acetabulum to the fossa on the head of the femur. In it, vessels and nerves pass to the head of the femur; the mechanical value of the ligament is insignificant.
Movement in the hip joint occurs around three axes: frontal - flexion and extension, sagittal - abduction and adduction, vertical - inward and outward rotation. In it, as in any triaxial joint, circular motion... The range of motion in the hip joint is less than in the triaxial shoulder joint, due to the fact that the head of the femur enters deeply into the glenoid cavity of the pelvic bone.
Knee-joint(articulatio genus) is formed by three bones: femur, tibia and patella (Fig. 53). The medial and lateral condyles of the femur are articulated with the condyles of the same name of the tibia, and the articular surface of the patella is adjacent to the front. The articular surfaces of the condyles of the tibia are slightly concave, and the articular surfaces of the condyles of the femur are convex, but their curvature is not the same. The discrepancy between the articular surfaces is compensated for by the medial and lateral menisci located in the joint cavity between the condyles of the articulating bones. The outer edge of the menisci is thickened, fused with the articular capsule. The inner edge is much thinner. The menisci are attached by ligaments to the intercondylar elevation of the tibia: their anterior edges are connected to each other by the transverse ligament of the knee. Menisci, being elastic formations, absorb shock transmitted from the foot when walking, running, jumping.
The anterior and posterior cruciate ligaments pass inside the joint cavity; connecting the femur and tibia. The synovial membrane of the articular capsule of the knee joint forms several inversions - synovial bursa (bursa), which communicate with the joint cavity. The larger is the patella, located between the tendon of the quadriceps femoris and the anterior surface of the distal end of the femur.
The knee joint strengthens strong external ligaments. The quadriceps femoris tendon attaches to the base of the patella and extends from the apex as the patellar ligament, which attaches to the tibial tuberosity. The tibial and peroneal collateral ligaments are located on the sides of the knee joint and extend from the epicondyle of the femur to the medial condyle of the tibia and to the head of the fibula, respectively.
The knee joint is a complex rotational block joint. V knee joint movements are carried out: flexion and extension of the lower leg, in addition, a slight rotational movement of the lower leg around its longitudinal axis. The last movement is possible when the lower leg is bent, when the collateral ligaments of the knee are relaxed.
Lower leg joints... The proximal ends of the shin bones are connected to each other through the tibiofibular joint, which is flat in shape. Between the bodies of both bones is the interosseous membrane of the lower leg. The distal ends of the tibia and fibula are connected using syndesmosis (ligaments), which are particularly durable.
Ankle joint(articulatio talocruralis) is formed by both bones of the lower leg and the talus (Fig. 54): the lower articular surface of the tibia and the articular surfaces of the ankles of both bones of the lower leg are articulated with the talus block. The joint is strengthened by the ligaments going from the bones of the lower leg to the talus, scaphoid and heel bones. The bursa is thin.
According to the shape of the articular surfaces, the joint is block-shaped. The movement takes place around the frontal axis: flexion and extension of the foot. Small side movements (adduction and abduction) are possible with strong plantar flexion.
Joints and ligaments of the foot... The bones of the foot are connected to each other through a series of joints reinforced with ligaments (see Fig. 54). Among the joints of the tarsus, the talocalcaneal-scaphoid and calcaneal-cuboid joints are of particular practical importance. They are collectively referred to as the transverse tarsal joint (known in surgery as the Chopard joint). This joint is reinforced on the dorsum of the foot with a bifurcated ligament - the so-called Chopard key. In the tarsal joints, supination and pronation of the foot, as well as adduction and abduction, are possible.
The joints of the tarsus to the metatarsus form the tarsometatarsal joints (known as the Lisfranc joint). On the back and plantar sides, they are reinforced with ligaments. Of these, the most durable medial interosseous tarsometatarsal ligament, called the Lisfranc key. The tarsometatarsal joints are flat joints, movements in them are insignificant,
The metatarsophalangeal and interphalangeal joints of the foot are similar in shape to those of the hand, but differ in a smaller range of motion. In the metatarsophalangeal joints, flexion and extension and slight movement to the sides occur, in the interphalangeal joints, flexion and extension.
The arch of the foot is strengthened by ligaments and muscles. Among the ligaments that strengthen the arch of the foot, the long plantar ligament plays the main role. Starting at the bottom surface of the calcaneus, it runs along the foot and fan-shaped to the base of all metatarsal bones and to the cuboid bone.
In the ilium, os ilium, two parts are distinguished: the lower, thickened part - the body, corpus ossis ilium, which participates in the formation of the acetabulum, acetabulum: the upper flat, thinned in the center - the wing, ala ossis ilium.
The border between the body and the wing is an arcuate line, well-defined on the inner surface of the bone, linea arcuata. The upper, thickened, free edge of the wing of the ilium is called the iliac crest, arista Uiaca. The edges of the scallop are pointed, rough; they are called lips - external, labium extermon, and internal, labium internum. Between them, along the scallop, there is a third roughness in the form of an intermediate line, Chpea intermedia.
All these formations are muscle attachment sites. abdominal wall and back. Crista iliaca ends in front with a well-defined protrusion, the anterior superior iliac spine, spina iliaca anterior superior. Below it, along the anterior edge of the wing, there is a notch, divided by the anterior lower spine, spina iliaca anterior inferior, into two parts. Of these, the upper, limited from above by spina iliaca anterior superior and from below by spina iliaca anterior inferior, is called a large iliac incision, incisura iliaca (Henie), or a lunar notch, incisura semilunaris. The lower small iliac notch, incisura iliaca minor (Henie), is located below the spina iliaca anterior inferior. She comes to the border with pubic bone, where there is a trace of fusion of both bones in the form of an ilio-scallop eminence, eminentia iliopectinea. At the posterior end of the crista iliaca is the posterior superior spine of the ilium, spina iliaca posterior superior, and somewhat lower, along the posterior edge of the wing, there is the posterior lower spine, spina iliaca posterior inferior.
The posterior edge of the wing of the ilium, lying below the spina iliaca posterior inferior, looks like a notch extending to the ischium - the large ischial notch, incisura ischiadica major. On the outer surface of the wing, ala ossis ilium, three rough lines are noticeable, which, according to the name of the gluteal muscles, starting within them, are called gluteal lines. lineae glutaeae. Of these, the lower, linea glutaea inferior, the shortest, stretches over the acetabulum; anterior, linea glutaea anterior, the longest, arcuately directed from incisura ischiadica major to spina iliaca anterior superior, and, posterior, linea glutaea posterior, is located in the posterior part of the wing of the ilium from spina iliaca posterior inferior to crista iliaca; having an almost vertical direction.
The inner surface of the wing of the ilium is smooth, evenly concave and is called fossa iliaca. In the posterior part of it, at the posterior end of the linea arcuata, there is an articular, which looks like auricle, ear-shaped surface, fades auricularis. With this surface, the ilium articulates with the sacrum bone. Around the circumference of the facies auricularis, a periarticular groove, sulcus raga-glenoidalis, is sometimes expressed. Above and posterior to the facies auricularis there is an iliac roughness, tuberositas iliaca, - the place of fixation of powerful ligaments.
The ilium is one of the largest bones in the human skeleton.... The right and left iliac bones are located in the upper-posterior parts of the pelvic bone.
The structure of the ilium
The ilium is paired. Therefore, both the left and right ilium have the same structure. They are divided into two parts: the body and the wing. The body is the short and thick section of the ilium. It merges with the ischium and pubic bones to form the acetabulum. Extended top part the ilium forms the wing. The curved upper edge of the wing is called the iliac crest. On the front of the ridge there are two small outgrowths - the lower and upper iliac spines. A little below them is the large ischial notch. The inner concave part of the wing forms the iliac fossa, and the convex outer part forms the gluteal surface. On the inner surface of the wing of the ilium there is an ear-shaped surface, which is the place of articulation of the sacrum and the pelvic bone.
Ilium fracture
Iliac fractures usually result from a direct impact or compression of the pelvic bones... In children, a fracture in the wing of the ilium can also occur as a result of a sharp contraction of the muscles of the buttocks. The symptoms of a fracture are:
- Severe tissue edema at the site of the fracture;
- Sharp pain, aggravated by any attempt to move the leg;
- A sharp decrease in the function of the lower limb on the side of the lesion, i.e. in case of injury to the right iliac bone, functions are impaired right leg, and in case of damage to the left - respectively left.
The fracture of the ilium is accompanied by significant hemorrhage, while the hematoma extends over the entire lateral surface of the pelvis and the upper third of the thigh. Tension of the muscles of the anterior abdominal wall is often observed.
If a fracture of the ilium is suspected, the victim should be taken to the hospital in the supine position. A small roller is placed under the knees. If the fracture is without displacement, then local anesthesia of the fracture area is performed, the leg is placed in a special splint and a strict bed rest for three to four weeks. For fractures with displacement, perform surgery, the purpose of which is to compare and fragments (reduction), after which the leg is placed in the splint and the injured patient is prescribed bed rest for a month. Then physiotherapy and massage are prescribed. Required classes physiotherapy exercises... Usually full recovery the function of the lower limb is observed 1.5 - 2 months after the abolition of bed rest. 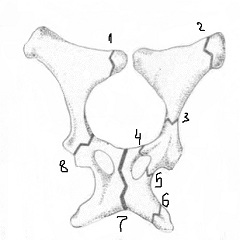
Iliac bone hurts: causes
In addition to injury, there are other reasons why the iliac bone hurts. They are quite diverse:
- High physical exercise when playing sports;
- Tumors of the ilium;
- Diseases of the blood (multiple myeloma, erythremia, chronic myeloid leukemia, acute leukemia, bone marrow diseases, Hodgkin's lymphoma);
- Infectious lesions of the ilium (tuberculosis, osteomyelitis);
- Metabolic bone diseases (deficiency of minerals and / or vitamin D, osteomalacia, vitamin B1 deficiency);
- Excessive secretion of cortisol, T3, or parathyroid hormone;
- Action of some drugs, in particular hormonal agents;
- Prolonged bed rest;
- The inhibition of osteoblast activity caused by age;
- Congenital collagen synthesis abnormality (Paget's disease).
In addition, pain in the right or left iliac bone can occur with osteochondrosis of the spine., herniated intervertebral discs. Therefore, if the iliac bone hurts, then you should not self-medicate, but you should see a doctor. Only a doctor, having done everything you need medical examination patient, will be able to find out true reason pain, make the correct diagnosis and prescribe the appropriate treatment.