The skeleton of the free upper limb is the hand. Fractures of the bones of the forearm
Normal human anatomy: lecture notes M. V. Yakovlev
6. SKELETON OF THE FREE UPPER LIMB. STRUCTURE OF THE HUMERUS AND BONES OF THE FOREARM. STRUCTURE OF THE BONES OF THE HAND
Brachial bone (humerus) has a body (central part) and two ends. The upper end passes into the head (capet humeri), along the edge of which the anatomical neck (collum anatomykum) passes. Behind the anatomical neck are large (tuberculum majus) and small tubercles (tuberculum minus), from which the crests of the same name (cristae tuberculi majoris et minoris) extend. Between the tubercles there is an intertubercular groove (sulcus intertubercularis).
Between the head and body of the humerus is the thinnest place of the bone - the surgical neck (collum chirurgicum).
In the lower half of the humerus, which has a trihedral shape, three surfaces are distinguished: medial, lateral and posterior. On the lateral surface there is a deltoid tuberosity (tuberositas deltoidea), below which the groove of the radial nerve (sulkus nervi radialis) passes. The distal end of the humerus ends with a condyle (condilus humeri), the medial part of which is represented by a block of the humerus (trochlea humeri), and the lateral part is the head of the condyle of the humerus (capitulum humeri). Above the block in front there is a coronary fossa (fossa coronaidea), and behind - a fossa of the olecranon (fossa olekrani). Above the head of the condyle is the radial fossa (fossa radialis). Above the condyles are elevations - epicondyles: medial and lateral. The medial epicondyle (epicondylus medialis) passes into the medial crest, which forms the medial edge of the humerus. On its posterior surface is the groove of the ulnar nerve (sulcus nervi ulnaris). The lateral epicondyle (epicondylus lateralis) passes into the lateral crest, forming the lateral edge.
To the bones forearms include the ulna and radius.
Radius(radius) has a body and two ends. The proximal end passes into the head of the radius (caput radii), on which there is an articular fossa (fovea artikularis). Under the head is the neck of the radius (collum radii), behind which is the tuberosity (tuberositas radii). The distal end has an ulnar notch (incisura ulnaris) on the medial side, and a styloid process (processus styloideus) on the lateral side. The lower surface of the distal end is represented by a concave carpal articular surface.
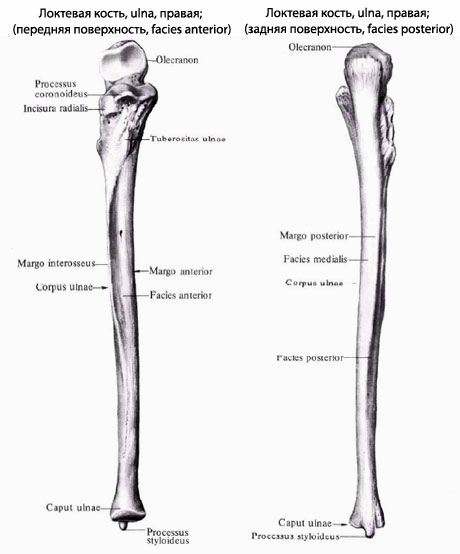
Elbow bone(ulna). At its proximal end there is a block-shaped notch (incisura trochlearis), ending with two processes: the ulnar (olecranon) and the coronal (processus coronoideus). On the coronoid process is the radial notch (incisura radialis), and just below this process is the tuberosity of the ulna (tuberositas ulnae). The distal end ends with a head (caput ulnae), from the medial side of which the styloid process (processus styloideus) departs. The head has an articular circumference (circumferencia articularis).
Brush(manus) consists of the bones of the wrist (ossa carpi), metacarpus (ossa metacarpi) and phalanges (phalanges) of the fingers.
Wrist(carpus) consists of eight bones arranged in two rows. The first row is formed by the pisiform (os pisiforme), trihedral (os triquetrum), lunate (os lunatum) and scaphoid (os scaphoideum) bones. The second row of bones are hook-shaped (os hamatum), capitate (os capitatum), trapezoid bones (os trapezoideum) and bone-trapezium (os trapezium).
metacarpal bones five. They distinguish the body (corpus metacarpale), the base (basis metacarpale) and the head (caput metacarpale).
phalanges fingers. All fingers, with the exception of the thumb, have three phalanges: proximal, middle and distal. In the phalanx, the body, base and head are distinguished.
From the book Traumatology and Orthopedics author Olga Ivanovna Zhidkova17. Fractures of the bones of the forearm Fractures of the olecranon occur more often when falling on the elbow. The fracture line penetrates the joint. Clinically, the fracture is expressed by local pain, swelling and hemorrhage, restriction of movement. Radiography clarifies
From the book Traumatology and Orthopedics author Olga Ivanovna Zhidkova18. Fractures of the bones of the hand A fracture of the navicular bone occurs when a person falls onto an extended hand. The fracture line often passes in the middle, narrowed part of the navicular bone, however, it is not always possible to detect a fracture radiographically in the first days after the injury. Usually
author Maxim Vasilievich Kabkov5. The structure of the bones of the cerebral region of the brain The skull (cranium) is a collection of tightly connected bones and forms a cavity in which vital organs are located. The cerebral region of the skull is formed by the occipital, sphenoid, parietal, ethmoid, frontal and temporal
From the book Normal Human Anatomy author Maxim Vasilievich Kabkov6. The structure of the bones of the facial section of the skull The body of the lower jaw (corpus mandibulae) has a lower (base (basis mandibulae)) and upper (alveolar (pars alveolaris)) parts, in the latter there are dental alveoli separated by interalveolar septa (septa interalveolaria). On the inside
From the book Normal Human Anatomy author Maxim Vasilievich Kabkov14. Muscles of the hand and auxiliary apparatus upper limb The middle group of muscles of the hand Palmar interosseous muscles (mm. interossei pa-lmares). Function: lead II, IV and V fingers to III. Dorsal interosseous muscles (mm. interossei dorsales). Function: remove II, IV and V fingers from III. Vermiform muscles (mm.
author Olga Ivanovna Zhidkova7. Intra-articular fractures of the bones of the forearm in the elbow joint. Fractures of the olecranon. Fractures of the olecranon occur more often when falling on the elbow. The fracture line penetrates the joint. Due to traction of the triceps muscle of the shoulder, the fragment is often displaced
From the book Traumatology and Orthopedics: Lecture Notes author Olga Ivanovna Zhidkova8. Diaphyseal fractures of the bones of the forearm Diaphyseal fractures of the bones of the forearm can occur with direct trauma. Fragments are displaced in width, length, at an angle and along the periphery. Particular attention is paid to the rotational displacement of fragments of the radius. In case of a fracture
From the book Traumatology and Orthopedics: Lecture Notes author Olga Ivanovna Zhidkova10. Fractures of the bones of the hand Fractures of the bones of the hand account for about a third of all bone fractures, of which phalangeal fractures account for 83%. Of the fractures of the bones of the wrist, the fracture of the navicular bone is in the first place, then the lunate and trihedral. Fracture of the scaphoid
author M. V. Yakovlev8. STRUCTURE OF THE SKELETON OF THE FREE PART OF THE LOWER LIMB. STRUCTURE OF THE FEMOR, PATELLET AND SHIN BONES. STRUCTURE OF THE BONES OF THE FOOT The femur (os femoris) has a body and two ends. The proximal end passes into the head (caput ossis femoris), in the middle of which is located
From the book Normal Human Anatomy: Lecture Notes author M. V. Yakovlev13. STRUCTURE OF THE BONES OF THE FACIAL SECTION OF THE SKULL The bones that form the facial skull include the upper and mandible, palatine bone, inferior turbinate, nasal bone, vomer, zygomatic, lacrimal and hyoid bones. The lower jaw (mandibula) has a body and branches. The body of the lower
From the book Normal Human Anatomy: Lecture Notes author M. V. Yakovlev4. JOINTS OF THE FREE UPPER LIMB Joints of the free upper limb (articulationes membri superioris liberi). The structure of the shoulder joint (articulatio humeri). The shoulder joint is the most mobile in the human body. The articular capsule is thin and free, has the shape of a truncated
From the book Normal Human Anatomy: Lecture Notes author M. V. Yakovlev6. STRUCTURE OF THE FREE LOWER LIMB JOINTS lower limb(articulationes membri inferioris liberi). The hip joint (articulatio coxae) refers to a variety of spherical joints - a cup-shaped type (articulatio cotylica). The acetabulum (labrum acetabulum) is firmly
From the book Normal Human Anatomy: Lecture Notes author M. V. Yakovlev7. AUXILIARY APPARATUS OF THE UPPER LIMB AND HAND MUSCLES
From the book Normal Human Anatomy: Lecture Notes author M. V. Yakovlev2. STRUCTURE OF THE MOUTH. STRUCTURE OF THE TEETH The oral cavity (cavitas oris) with closed jaws is filled with the tongue. Its outer walls are the lingual surface of the dental arches and gums (upper and lower), upper wall represented by the sky, the lower - by the muscles of the upper part of the neck, which
From the book Forensic Medicine. Crib author V. V. Batalina11. Mechanisms of occurrence of bone injuries under the action of blunt objects. Damage to the bones of the skull On the type of bones, the nature of the damaging object, on the strength and speed of the traumatic effect, as well as on the direction of the force in relation to the damaging
From the book Atlas: human anatomy and physiology. Complete practical guide author Elena Yurievna ZigalovaBones and joints of the bones of the limbs The function of the human limbs is clearly delineated: the upper ones are the organ of labor, the lower ones are supports and movements. This leaves a significant imprint on their structure. Limbs are a system of levers having a similar plan
17. Bones of the shoulder and forearm
The shoulder contains only one bone - the humerus. The humerus is a typical tubular bone. Its body in the upper section has a rounded cross-section, and in the lower section it is trihedral.
At the upper end (proximal epiphysis) of the humerus is the head of the humerus. It has the shape of a hemisphere, facing the scapula and bears the articular surface, to which the so-called anatomical neck of the humerus adjoins. Outside the neck are two tubercles that serve to attach muscles: a large tubercle, facing outward, and a small tubercle, facing anteriorly. A ridge descends from each of the tubercles. Between the tubercles and ridges there is a groove in which the tendon of the long head of the biceps brachii passes. Below the tubercles is the most narrowed place of the humerus - its surgical neck.
On the outer surface of the body (diaphysis) of the humerus there is a deltoid tuberosity, to which the deltoid muscle is attached. With the development of the deltoid muscle as a result of sports training, not only an increase in deltoid tuberosity is observed, but also an increase in the thickness of the entire compact bone layer in this area. On the posterior surface of the body of the humerus, the furrow of the radial nerve runs spirally from top to bottom and outwards.
The lower end (distal epiphysis) of the humerus forms the condyle and has an articular surface that serves to articulate with the bones of the forearm. The medial part of the articular surface, articulating with the ulna, is called the humeral block, and the lateral, articulating with the radius, has a spherical shape and is called the head of the condyle of the humerus. Above the block, in front and behind, there are pits, into which, when the forearm is flexed and unbent, processes of the ulna enter - coronal (front) and ulnar (rear). These fossae bear the corresponding names: the anterior - the coronary fossa and the posterior - the fossa of the olecranon. On both sides of the distal end of the humerus, there are medial and lateral epicondyles, easily palpable under the skin, especially the medial one, which has a groove for the ulnar nerve on its back side. The epicondyles serve to attach muscles and ligaments.
Forearm bones
The bones of the forearm are long tubular bones. There are two of them: ulna, ulna, lying medially, and radial radius located on the lateral side. The bodies of both bones have a trihedral shape with three surfaces and three edges. One surface is back, the other is front and the third is radii - lateral, in ulna - medial. Of the three edges, one is sharp. It separates the anterior surface from the posterior and faces the adjacent bone, limiting the interosseous space, which is why it is called margo interossea. On the front surface of the body there is a vascular opening, foramen nutricium (diaphyseos), leading to the same canal for blood vessels. In addition to these features common to both bones, there are a number of features for each bone separately.
Elbow bone
Ulna, ulna. The upper (proximal) thickened end of the ulna (pineal gland) is divided into two processes: posterior, thicker, olecranon, olecranon, and front, small, coronoid, processus coronoideus. Between these two branches is block notch, incisura trochlearis, serving for articulation with the block of the humerus. On the radial side of the coronoid process is placed a small incisura radialis- the place of articulation with the head of the radius, and in front under the coronoid process lies tuberosity, tuberositas ulnae, the place of attachment of the tendon m. brachialis. The lower (distal) end of the ulna bears a round, with a flat lower head surface, caput ulnae (epiphysis), from which the medial side departs (apophysis). The head has around its circumference articular surface, circumferentia articularis, the place of articulation with the neighboring radius.
Radius, radius. In contrast, the ulna has a more thickened distal end than the proximal end. The proximal end forms a rounded head, caput radii (pineal gland), with a flat recess for articulation with capitulum humeri. One third or half of the circumference of the head is also occupied articular surface, circumferentia articularis attached to incisura radialis ulna. The beam head is separated from the rest neck bones, collum radii, immediately below which on the anterior ulnar side tuberosity stands out, tuberositas radii(apophysis), the place of attachment of the biceps of the shoulder. The lateral edge of the distal end (epiphysis) continues into styloid process, processus styloideus(apophysis). Located on the distal epiphysis articular surface, facies articularis carpea, concave for articulation with the scaphoid and lunate bones of the wrist. On the medial edge of the distal end of the beam there is small tenderloin, incisura ulnaris, the place of articulation with the circumferentia articularis of the head of the ulna.
Ossification. The distal part of the humerus and the proximal parts of the bones of the forearm develop due to separate ossification points that occur in six points: in the epiphyses (capftulum humeri - on the 2nd year, caput radii - on the 5th -6th year, olecranon - on the 8th - 11th year, trochlea - in the 9th - 10th year) and apophyses (epicondylus medialis - in the 6th -8th year and lateralis - in the 12th - 13th year) (Fig. 44). In trochlea and olecranon, the ossification points are multiple. Therefore, on the radiograph of the elbow joint in childhood and adolescence, there is big number bone fragments, the presence of which complicates the differential diagnosis between the norm and pathology. Because of this, knowledge of the features of ossification of the elbow joint area is mandatory. By the age of 20, synostosis sets in. In case of non-fusion of the olecrani bone nucleus with the ulna, it may remain in an adult unstable bone, os sesamoideum cubiti, or patella cubiti.
FOREARM [antebracium(PNA, JNA); antibrachium (BNA)] - the middle segment of the upper limb.
Anatomy
Rice. Fig. 1. The relief of the muscles and external landmarks of the anatomical formations of the anterior-external (a), anterior-internal (6), posterior (c) surfaces of the male forearm: 1 - tendon of the long extensor of the thumb; 2 - short extensor of the thumb; 3 - a long muscle that removes the thumb; 4 - tendon of the radial flexor of the wrist; 5 - tendon of the long palmar muscle; 6 - tendon of the long radial extensor of the wrist; 7 - brachioradialis muscle; 8 - biceps muscle of the shoulder; 9 - round pronator; 10 - shoulder muscle; 11- neurovascular bundle; 12- medial head of the triceps muscle of the shoulder; 13 - medial epicondyle; 14 - olecranon; 15 - tendon of the biceps muscle of the shoulder; 16 - radial flexor of the wrist; 17 - superficial finger flexor; 18 - tendon of the ulnar flexor of the wrist; 19 - tenar (elevation of the thumb); 20 - distal skin fold wrists; 21 - tendon of the brachioradialis muscle; 22 - elbow flexor of the wrist; 23 - proximal skin fold of the wrist; 24 - styloid process of the ulna; 25 - average skin fold of the wrist; 26 - hypothenar (elevation of the little finger); 27 - lateral epicondyle; 28 - long radial extensor of the wrist; 29 - extensor of the fingers; 30 - elbow extensor of the wrist; 31 - short radial extensor of the wrist; 32 - extensor of the little finger; 33 - posterior edge of the ulna 34 - medial saphenous vein of the arm; 35 - elbow muscle.
Borders: upper circular line drawn 5-6 cm below the epicondyles of the humerus; the lower one runs along a circular line connecting the tops of the styloid processes of the ulna and radius bones. When examining P., many of the bone and soft tissue formations of this segment are visible (Fig. 1).
Rice. 2. Bones and ligaments of the right forearm (front view): 1- olecranon of the ulna; 2 - block-shaped notch of the ulna; 3 - tuberosity of the ulna; 4 - oblique chord; 5 - articular capsule of the distal radioulnar joint; b - styloid process of the ulna; 7 - styloid process of the radius; 8 - interosseous membrane of the forearm; 9 - tuberosity of the radius; 10 - annular ligament of the radius; 11 - head of the radius; 12 - coronoid process of the ulna.
The bone base of P. is made up of the radius and ulna. The epiphyses of the bones are connected to each other by the proximal and distal radioulnar joints (articulationes radioulnares proximalis et distalis), which makes it possible to move the radius around the ulna outward (supination) and inwards (pronation). The epiphyses of the radius and ulna are reinforced with ligaments, the diaphyses are connected by an oblique chord and the interosseous membrane P. (Fig. 2). The skin on P. is thin, mobile, with hairline on the back and side surfaces. Own fascia, giving fascial partitions to the bones of P., forms fascial beds: anterior, external and posterior. The muscles are separated from each other by fascial spurs of their own fascia. At the top, the fascia is strengthened by the aponeurosis of the biceps muscle (aponeurosis m. bicipitis brachii), and below by the flexor and extensor retinaculums (retinaculum flexorum et extensorum). In the anterior fascial bed, the anterior muscle group is located in four layers: the first layer is the round pronator (m. pronator teres), the radial flexor of the wrist (m. flexor carpi radialis), the long palmar muscle (m. palmaris longus); the second is the superficial flexor of the fingers (i.e. flexor digitorum superficialis); the third is a deep flexor of the fingers (m. flexor digitorum profundus), a long flexor of the first finger of the hand (t. flexor pollicis longus); the fourth is a square pronator (m. pronator quadratus). Between the second and third layers is the anterior intermuscular cellular gap; between the third layer and the interosseous membrane - the anterior interosseous-muscular cellular fissure; between the square pronator, the interosseous membrane and both P.'s bones - Pirogov's space. In the outer fascial bed there is an external group of muscles: brachioradialis (m. brachioradialis), long and short radial extensor wrists (m. extensor carpi radialis longus et brevis). In the posterior fascial bed lies in two layers rear group muscles: the first layer is the ulnar muscle (m. anconeus), the ulnar extensor of the wrist (m. extensor carpi ulnaris), the extensor of the V finger (m. extensor digiti minimi), the extensor of the fingers (m. extensor digitorum); the second layer is the supinator (m. supinator) in the upper third and below - the extensor of the second finger (m. extensor indicis) and the initial sections of the short and long extensor of the first finger of the hand (mm. extensores pollicis longus et brevis), the long muscle that abducts the first finger brushes (m. abductor pollicis longus); between the first and second layers is the posterior intermuscular gap; between the second layer, the interosseous membrane and both bones, there is a posterior interosseous-muscular cellular fissure. The supinator canal (canalis supinatorius) is a slit-like gap between the radius and the arch support. A deep branch of the radial nerve (m. profundus n. radialis) passes through it. The anterior muscle group flexes the fingers and hand and pronates the forearm; external and back - unbends the fingers and hand and supinates the forearm.
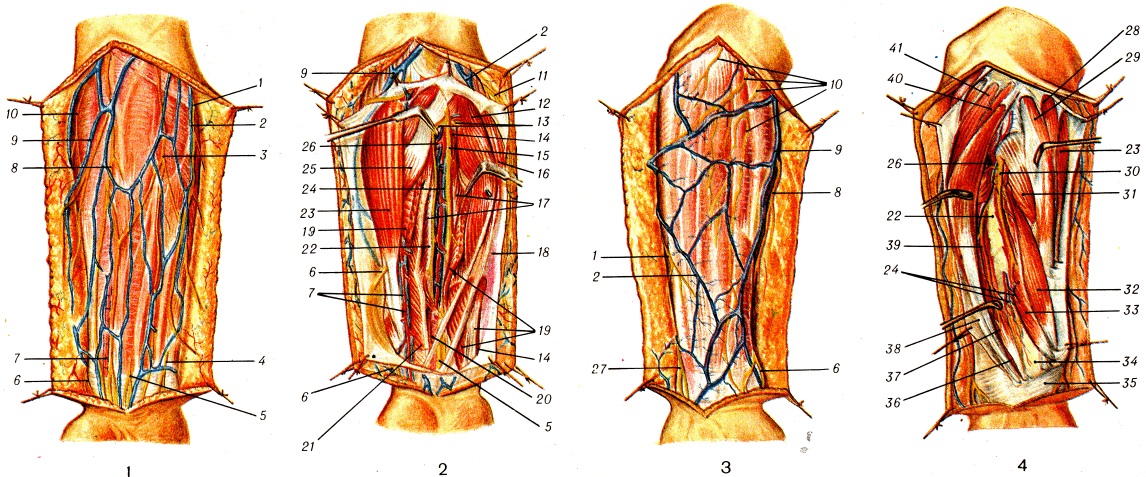
Color illustrations. Rice. one. Superficial veins and nerves of the anterior region of the forearm (skin and partially subcutaneous tissue are separated). Rice. 2. Muscles, nerves, vessels and anterior interosseous neurovascular bundle of the anterior region of the forearm (skin, subcutaneous tissue and fascia of the forearm were separated, the muscles were partially dissected and moved apart). Rice. 3. Superficial veins and nerves of the posterior region of the forearm (skin and partially subcutaneous tissue are separated). Rice. 4. Muscles, nerves and vessels of the posterior region of the forearm (skin, subcutaneous tissue and fascia of the forearm were separated). 7-ulnar branch of the medial cutaneous nerve of the forearm; 2 - medial saphenous vein of the arm; 3- anterior branch of the medial cutaneous nerve of the forearm; 4 - palmar branch of the ulnar nerve; 5 - palmar branch of the median nerve; 6-superficial branch of the radial nerve; 7-beam artery and vein; 8 - lateral cutaneous nerve of the forearm; 9 - lateral saphenous vein of the arm; 10 - posterior cutaneous nerve of the forearm; 11 - medial cutaneous nerve of the forearm; 12 - radial flexor of the wrist; 13 - muscular branches of the median nerve; 14 - ulnar artery; 15 - median nerve; 16 - long palmar muscle; 17 - deep finger flexor; 18 - elbow flexor of the wrist (covered by fascia); 19 - superficial finger flexor; 20 - square pronator; 21-long flexor of the thumb; 22 - interosseous membrane of the forearm; 23 - brachioradialis muscle; 24 - anterior interosseous neurovascular bundle; 25 - round pronator; 26 - posterior interosseous artery; 27-dorsal branch of the ulnar nerve; 28 - long radial extensor of the wrist; 29 - short radial extensor of the wrist; 30 - deep branch of the radial nerve; 31 - arch support; 32 - a long muscle that removes the thumb; 33 - short extensor of the thumb; 34 - radius; 35 - extensor retinaculum; 36 - extensor index finger; 37 - long extensor of the thumb; 38 - extensor of the fingers; 39 - posterior interosseous nerve; 40 - extensor of the little finger; 41 - ulnar extensor of the wrist.
In the subcutaneous tissue of P. there are medial (v. basilica) and lateral (v. cephalica) superficial veins, as well as the median vein of P. (v. mediana antebrachii) and their tributaries (tsvetn. ill., Fig. 1.3). deep veins Items (vv. commitentes) accompany arteries. The anterior and lateral surfaces of P. are innervated by the medial and lateral cutaneous nerves of P. (nn. cutanei antebrachii med. et lat.), the posterior - by the posterior cutaneous nerve of P. (n. cutaneus antebrachii post.). On P., it is possible to distinguish the radial, ulnar, anterior and posterior interosseous neurovascular bundles and the median nerve (tsvetn. ill., Fig. 2.4). The radial artery and veins, the superficial branch of the radial nerve (a. et vv. radiales, r. superficialis n. radialis) are located between the radioulnar muscle and the radial flexor of the wrist. The ulnar artery, veins and nerve (a., vv. et n. ulnares) in the lower 2/3 of the forearm pass between the ulnar flexor of the wrist and the deep flexor of the fingers, and in the upper third the ulnar artery lies outward from the nerve on the deep flexor of the fingers. The anterior and posterior interosseous arteries (aa. interosseae ant. et post.) with the veins and nerves of the same name pass along the anterior and posterior surfaces of the interosseous membrane; median nerve (n. medianus) - between the deep and superficial flexors of the fingers. The anterior muscle group is innervated by the median and partially ulnar nerves, the external and posterior by the radial nerve.
Lymph. P.'s vessels are formed from limf, muscle capillaries, fascias, subcutaneous tissue and skin. They carry lymph to the elbow and axillary nodes.
1 - styloid process of the radius: 2 - tuberosity of the radius; 3 - neck of the radius; 4- head of the radius: 5 - olecranon of the ulna; 6 - coronoid process of the ulna; 7 and 8 - interosseous crests of the radius and ulna; 9 - ulnar notch of the radius; 10 - styloid process of the ulna.
X-ray anatomy
Pictures of the diaphysis of the bones of the forearm are made in direct and lateral (ulnar) projections, according to indications, in oblique projections. The diaphyses of the radius and ulna are not sharply arcuately curved (Fig. 3). The thickness of the ulna in the distal direction decreases, and the radius, on the contrary, increases. The width of the compact substance is not the same, it has the greatest density and thickness on the adjacent surfaces of the bones of the forearm, that is, adjacent to the interosseous membrane. The most thickened areas of the cortex are called ridges. Due to their uneven density, they are sometimes mistaken for periostitis. The lumen of the medullary canal is clearly differentiated along the diaphysis of the bones. Oblique lines of enlightenment crossing the cortical substance are a reflection of the nutrient channels.
Pathology
Malformations are rare. These include: hemimelia - complete absence entire forearm; phocomelia - underdevelopment of the shoulder and P., when the hand starts directly from the body; peromelia - the complete absence of the entire upper limb, when an insignificant rudiment departs from the body. Congenital absence or underdevelopment of the radius or ulna is often symmetrical and entails congenital clubhand (see).
Congenital dislocation of the radius develops on the basis of patol. shortening of the ulna with a normal length of the radius. The head of the radius is usually deformed, which is the reason for the restriction of rotation, flexion and extension of the P. Treatment is surgical - resection of the head of the radius in patients over 14 years of age.
P.'s malformations also include congenital radioulnar synostosis (see Elbow joint), Madelung's disease (see Madelung's disease).
Damage Items can be closed and open. Closed injuries include bruises (see), ruptures of muscles and tendons (see Distortion, Muscles), as well as bone fractures (see Fractures). With significant subfascial hematomas due to P.'s bruises, compression of blood vessels, nerves and muscles is possible, which is manifested by ischemia, impaired skin sensitivity and hand function. In these cases, an incision of the skin and fascia and removal of the hematoma are indicated. Subcutaneous ruptures of the muscles and tendons of P. are rare.
They can be complete or partial. Diagnostic features is local pain, hematoma, dysfunction of the hand or fingers. With partial damage, conservative treatment is indicated. Complete breaks are subject to surgical treatment with suturing on the damaged muscle or tendon.
At wounds of soft tissues of P. make primary surgical treatment of wounds (see).
Fractures of the bones of the forearm among all bone fractures range from 5 to 25%. They can be open and closed.
Fractures of the head of the radius, olecranon, coronoid process of the ulna - see Elbow joint.
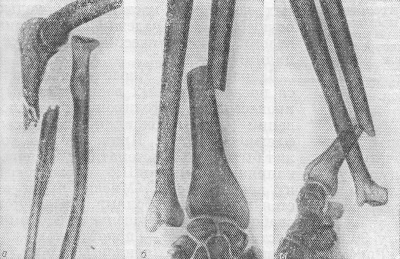
A - comminuted fracture of the ulna in the proximal third with dislocation of the head of the radius; b - fracture of the radius in the middle third with dislocation of the head of the ulna; c - fracture of the radius, dislocation and fracture of the head of the ulna (a variant of the Galeazzi fracture).

Fractures of the diaphysis of P.'s bones occur when exposed to direct or indirect trauma. Fractures can be in the upper, middle and lower third of the P.'s bones, one radius, one ulna, both P.'s bones, the diaphysis of the ulna with dislocation of the radial head - Monteggi's fracture (Fig. 4, a), the diaphysis of the radius with dislocation of the head ulna - Galeazzi fracture (Fig. 4, b, c). Diaphyseal fractures of P.'s bones are transverse, oblique, comminuted, fragmented. Possible displacement of fragments in width, length, at an angle and rotational displacement. In children, subperiosteal fractures occur more often (Fig. 5) - according to the “green branch” type, when the preserved periosteum holds bone fragments and therefore their displacement is not pronounced.
As a result of injury, epiphysiolysis can occur, which is more common in the distal radius. The degree of displacement of the epiphysis varies - from a slight asymmetric expansion of the zone of the metaepiphyseal cartilage to displacement of the epiphysis by half or more of the diameter of the bone. As a rule, together with the epiphysis, a small bone fragment that breaks away from the metaphysis (osteoepiphysiolysis) is displaced.
A fracture of the distal end of the radius (a fracture in a typical location) occurs at the site of the former growth zone (2-2.5 cm from the joint space), the peripheral fragment of the radius is displaced to the back of the P. - a Collis fracture (see Collis fracture); when falling on the back surface of the hand, the peripheral fragment is displaced to the palmar side (Smith's fracture).
With isolated injuries of individual bones, local symptoms fracture - local pain, violation of the form and function of P. and the hand (see Fractures). Pay attention to the state of the distal (with a fracture of the radius) and proximal (with a fracture of the ulna) radioulnar joints, since dislocation of the bones is possible. When conducting radiography, pictures are taken in two projections with the capture of the elbow and wrist joints.
With closed fractures of both bones, P. without displacement of fragments is applied for 2-2.5 months. a plaster cast in P.'s position, average between pronation and supination, with elbow flexion up to 90°. At closed P.'s fractures with displacement of fragments, they are repositioned (see), after which a circular plaster cast is applied (see Plaster technique). X-ray. control is carried out immediately after reposition, as well as 10-14 days after it, after the cessation of tissue edema. The period of immobilization with a plaster bandage is 2.5 - 3 months. Ability to work is restored after 4-5 months. after fracture. With isolated fractures of P.'s bones, the tactics are the same.
Osteosynthesis is used for unsuccessful closed reposition, secondary displacements in the plaster cast, as well as for Monteggi and Galeazzi fractures. The most common is extraosseous or intraosseous osteosynthesis of the bones of the forearm (see Osteosynthesis). In case of a Monteggi fracture, the dislocation of the head of the radius is reduced and it is temporarily fixed transosseously with a pin, and then osteosynthesis of the fragments of the ulna is performed. With chronic dislocations of the head of the radius, its resection is indicated. In case of a Galeazzi fracture, osteosynthesis of the radius is carried out with a plate, the dislocation of the head of the ulna is reduced. After osteosynthesis for 2.5-3 months. apply a plaster circular bandage. In case of bone fractures, P. may develop severe complication- Volkmann's contracture (see Contracture).
Open fractures of P.'s bones occur with direct trauma from the outside (often comminuted and crushed fractures), as well as as a result of puncture of soft tissues and skin from the inside by the sharp ends of fragments.
In the case of open fractures of P.'s bones without displacement of fragments, and also after successful reposition of fragments, a split circular or longet plaster bandage is applied. Submersible osteosynthesis with metal structures can be carried out during surgical treatment of a wound with a small area of soft tissue damage, in the absence of signs of inf. complications and, if possible, suturing the wound. With multifragmented and crushed fractures, as well as with extensive P.'s wounds, it is more appropriate to fix fragments with devices for transosseous fixation (see Distraction-compression devices).
In the treatment of P.'s fractures, in addition to the immobilization of fragments, a large role belongs to therapeutic gymnastics. This is due to the fact that the consequences of P.'s injuries, especially bone fractures, adversely affect the function of the hand. After applying a plaster bandage on the 2-3rd day, movements begin in the joints of the hand, free from the plaster bandage. Perform various finger movements (flexion and extension, dilution and reduction, opposition), movements along all axes of the shoulder joint. For the muscles under the cast, exercises are used that include static stress followed by relaxation. After the termination of immobilization by the injured hand in its initial position on the surface of the table, the patient performs exercises for the fingers, movements in the wrist joint, pronation and supination of the P., movements in the elbow joint. good effect give exercises in warm water in the form of active movements with a brush and fingers. With long-lasting swelling of the hand, a light massage of the forearm is shown. At the end of treatment, rubber bandages, dumbbells, expanders are used to further increase the range of motion in the joints and strengthen the muscles of the hand. To speed up the recovery of working capacity, occupational therapy is widely used (screwing bolts with a screwdriver, working with a plane and a saw, winding threads on a ball, gluing envelopes, etc.).

Features of combat damage, staged treatment. When applied modern species weapons, gunshot wounds to P., injuries caused by a shock wave (closed and open fractures of bones, compression, etc.), as well as combined injuries, can be observed. P.'s injuries are classified according to the type of wounding projectile, the nature and localization of the wound, the type of fracture, the degree of destruction of soft tissues, as well as concomitant injuries. Gunshot fractures of P.'s bones during the Great Patriotic War accounted for 36.7% of gunshot fractures of long tubular bones. Damage to vessels associated with P.'s fractures was in 7.4%, nerves - in 30.5% of the wounded. P.'s wounds by small-caliber bullets with a high initial flight speed are accompanied by extensive destruction of soft tissues in the region of the exit hole, multi-comminuted bone fractures, often with a defect in bone tissue (Fig. 6).
At diagnosis of P.'s changes take into account: P.'s deformation, an arrangement of entrance and exit openings and the direction of the wound channel, presence of bone fragments visible in a wound, patol. mobility at the level of injury, pain in the fracture area, limitation of active and passive movements of the hand and fingers. The final diagnosis is established after carrying out rentgenol, researches.
First health care: stopping bleeding with a pressure bandage or tourniquet, applying an aseptic bandage, immobilizing P. with improvised means, administering analgesics.
Before medical assistance: control and correction of applied bandages, splints and hemostatic tourniquets, the introduction of analgesics, according to indications, improvement of immobilization with wire or plywood splints.
First medical aid: correction or replacement of dressings, splints and hemostatic tourniquets, temporary stop of bleeding - ligation of a damaged vessel or clamping it in a wound with a hemostatic clamp, administration of analgesics, antibiotics, tetanus toxoid and tetanus toxoid.
Qualified medical care is usually provided for urgent indications (continued bleeding, detachment and crushing of the limb, anaerobic infection).
Specialized medical care: surgical treatment of the wound and reliable immobilization of fragments with a plaster bandage, according to indications during surgical treatment, economical resection of fragments of comminuted and comminuted fractures of the P. bones in order to securely fix the fragments with metal structures.
Diseases. Myositis develops after various inflammatory processes and infectious diseases(influenza, tonsillitis, abscesses, phlegmon, etc.). The reason for it can also be a systematic overstrain of the P.'s muscles, causing their overwork. Myositis is manifested by persistent pain, muscle weakness and dysfunction of the hand. Treatment - rest, novocaine blockade, thermal procedures, superficial massage. In cases of a persistent course of myositis, P.'s immobilization is used (see Myositis).
Aseptic tendovaginitis of tendons P. may occur with severe physical labor. More often this process affects the extensor of the fingers and the radial and ulnar extensors of the wrist. Treatment - two- or three-time irrigation with chlorethyl of the skin along the interested tendon with an interval of 2-3 days; peace and warmth. Acute purulent tendovaginitis of the flexors of the fingers, which is usually a complication of panaritium (see), may be accompanied by purulent fusion of tissues and a breakthrough of pus into Pirogov's space. Treatment operational (see. Tendovaginitis ).
Osteomyelitis can be hematogenous and post-traumatic (as a complication of gunshot or open non-gunshot fractures) or postoperative. Hematogenous osteomyelitis of P.'s bones occurs less frequently than other bones of the skeleton. The metaphyseal part of the bones is more often affected, less often the diaphyseal. Treatment is carried out according to the principles adopted for the treatment of osteomyelitis (see Osteomyelitis, treatment).
Tuberculosis usually occurs with damage to the epiphyseal and metaphyseal parts of P.'s bones (see Extrapulmonary tuberculosis).
Syphilitic osteoperiostitis of P.'s bones is more often asymmetric, with focal parietal usura. Great importance at recognition have data a wedge. paintings and lab. research. Specific treatment (see Syphilis).
Mycoses (actinomycosis, spirotrichosis, aspergillosis, etc.) rarely affect P.'s bones (see Mycoses).
In P.'s bones, changes can be observed in hyperparathyroidism, Paget's disease, a localized cyst and osteoblastoclastoma occur (see Bone cyst, Osteoblastoclastoma, Parathyroid osteodystrophy, Paget's disease).
After damage and various diseases muscles and tendons of P., as well as after fractures of P.'s bones, contractures of the hand and fingers, rotational contracture of P. may occur, special form contractures - Volkmann's (see (see), chondromyxoid fibroma, (see), myeloma, bone reticulosarcoma (see Primary bone reticulosarcoma) in the P. area, as well as metastases malignant tumors are rarely observed. Treatment is usually surgical, followed by radiation therapy. AT early stages savings operations are possible - wide resections of P.'s bones with bone alloplasty. AT late stages shown amputation at shoulder level. The prognosis for life is determined by the timeliness of the treatment; in savings operations, the P. function in to a large extent is being restored.
Operations
Access to the diaphysis of the radius can be carried out along the outer, palmar or dorsal side of P.; access to the diaphysis of the ulna - along the inner, palmar plate on the back side of the P. The ulnar artery and ulnar nerve are exposed using palmar-ulnar access. A skin incision with supinated P. is made from the medial epicondyle of the shoulder to the outer edge of the pisiform bone. After dissection of the fascia, the ulnar artery and ulnar nerve are found in the gap between the ulnar flexor of the hand and the superficial flexor of the fingers. The radial artery and the superficial branch of the radial nerve are exposed using palmar radial access. The skin incision is made with the supinated position of P. along the line connecting the outer edge of the tendon of the biceps muscle of the shoulder and the styloid process of the radius. The artery and superficial branch of the radial nerve are exposed between the pronator teres and the brachioradialis muscle.
P.'s amputation in the upper and middle thirds is carried out in a patchwork or circular manner with a cuff. The median, ulnar and radial nerves are shortened by 4-5 cm in order to exclude the possibility of the formation of an amputation neuroma under the skin at the end of the stump. Muscles and tendons are crossed in the same plane 3-4 cm distal to the sawdust of the bones. P.'s bones are filed at the same level, their edges are smoothed with a rasp. The vessels are tied up with catgut (see Amputation). According to the indications, kinematization of the stump is carried out (see Krukenberg's hand). P.'s bones resection is carried out at tumors, in some cases osteomyelitis and false joints.
Elongation of P.'s bones is indicated for clubhand (see), congenital and acquired shortenings. After oblique osteotomy, lengthening is performed using distraction-compression devices. The osteotomy in the P.'s area is similar according to indications and equipment of an osteotomy of other long tubular bones (see. Osteotomy ).
Bibliography:
Kaplan A.V. Damage to bones and joints, p. 252, M., 1979; Kaptelin A.F. Rehabilitation treatment (physiotherapy, massage and occupational therapy) for injuries and deformities of the musculoskeletal system, M., 1969; Clinical radioanatomy, ed. G. Yu. Koval, p. 199, Kyiv, 1975; To islands of V. V. and Travin A. A. Surgical anatomy of upper extremities, M., 1965; Maykova-Stroganova V. S. and Rokhlin D. G. Bones and joints in the x-ray image, Extremities, p. 331, JI., 1957; Multi-volume guide to orthopedics and traumatology, ed. N. P. Novachenko, vol. 1, p. 389, M., 1967, v. 2, p. 483, 515, Moscow, 1968; Nagy D. X-ray anatomy, trans. from Hungarian, p. 74, Budapest, 1961; Operative surgery and topographic anatomy, ed. V. V. Kovanova, p. 29, M., 1978; The experience of Soviet medicine in the Great Patriotic War 1941-1945, v. 15, p. 276, M., 1952; Essays on military field surgery, ed. Yu. G. Shaposhnikova. Moscow, 1977. Reinberg S. A. X-ray diagnostics of diseases of bones and joints, book. 1-2, M., 1964; Rubasheva A. E. Private radiodiagnosis of diseases of bones and joints, Kyiv, 1967; Chernavsky V. A. Diagnosis and treatment of fractures and dislocations, p. 96, Tashkent, 1977; Bensahel H. Fractures de Monteggia, Rev. Prat., v. 22, p. 1679, 1972; Boileau F., Pre-aut J. et Malka G. Les fractures diaphysaires récentes de l'avant-bras chez l'adulte, Ann. Med. Nancy, t. 12, p. 2257, 1973, bibliogr.; Brug E., Beck H. u. Heuwieser R. Osteosynthese son Unterarmschaftfrakturen mit dem Bündelnagel nach Hackethal, Chirurg, Bd 46, S. 113, 1975; Christensen N. O. Küntscher intramedullary reaming and nail fixation for nonunion of the forearm, Clin. Orthop., v. 116, p. 215, 1976; E a t o n R. G. a. G r e e n W. T. Volkmann's ischemia, A volar compartement syndromè of the forearm, ibid., v. 113, p. 58, 1975; E r 1 e r F. Osteosynthesen bei Unterarmbrüchen, Beitr. Orthop. Trau-mat., Bd 23, S. 132, 1976; F i n k b e i-n e r G. F. u. Hort W. Therapie der anbehandelten Unterarmfrakturen, Z. Orthop., Bd 114, S. 666, 1976; L a n z T. u. Wachsmuth W. Praktische Anatomie, Bd 1, B., 1959; Lukacs L. u. Törtely E. Komplikationen nach Verplattung von Unterarmbrüchen, Akt. Traumatol., Bd 6, S. 221, 1976.
C. S. Tkachenko; V. P. Illarionov (to lay down. physical.), M. K. Klimova (rents.), E. R. Mattis (hir.), A. A. Travin (An.).
They belong to long tubular bones. There are two of them: the ulna, ulna, lying medially, and the radial radius, located on the lateral side. The bodies of both bones have a trihedral shape with three surfaces and three edges. One surface is posterior, the other is anterior, and the third in radii is lateral, in ulna is medial. Of the three edges, one is sharp.
It separates the anterior surface from the posterior and faces the adjacent bone, limiting the interosseous space, which is why it is called margo interossea. On the front surface of the body there is a vascular opening, foramen nutricium (diaphyseos), leading to the same canal for blood vessels. In addition to these features common to both bones, there are a number of features for each bone separately.
Which doctors to contact for examination of the bones of the forearm:
Traumatologist
What diseases are associated with the bones of the forearm:
What tests and diagnostics need to be done for the bones of the forearm:
X-ray of the forearm
Are you worried about something? Do you want to know more detailed information about the bones of the forearm or do you need an examination? You can book an appointment with a doctor– clinic Eurolaboratory always at your service! The best doctors examine you, advise, provide needed help and make a diagnosis. you also can call a doctor at home. Clinic Eurolaboratory open for you around the clock.
How to contact the clinic:
Phone of our clinic in Kyiv: (+38 044) 206-20-00 (multichannel). The secretary of the clinic will select a convenient day and hour for you to visit the doctor. Our coordinates and directions are indicated. Look in more detail about all the services of the clinic on her.
If you have previously performed any research, be sure to take their results to a consultation with a doctor. If the studies have not been completed, we will do everything necessary in our clinic or with our colleagues in other clinics.
You need to be very careful about your overall health. There are many diseases that at first do not manifest themselves in our body, but in the end it turns out that, unfortunately, it is too late to treat them. To do this, you just need to several times a year be examined by a doctor not only to prevent a terrible disease, but also to maintain healthy mind in the body and the body as a whole.
If you want to ask a doctor a question, use the online consultation section, perhaps you will find answers to your questions there and read self care tips. If you are interested in reviews about clinics and doctors, try to find the information you need on. Also register for medical portal Eurolaboratory to be constantly up to date latest news and updates of information about the bones of the forearm on the site, which will be automatically sent to you by mail.
Other anatomical terms on the letter "K":
| Brush |
| Foreskin (prepuce) |
| Clitoris |
| Knee-joint |
| Blood |
| Intestines |
| Blood vessels |
| telencephalon |
| Bone |
| Bone labyrinth |
| Cell |
| Adam's apple (Adam's apple) |
| blood capillaries |
| capillaries |
| Bone |
| Lower leg bones |
| Foot bones |
| Collarbone |
| coccygeal vertebrae |
| Coccyx |
| Sacrum |
| wrist bones |
| Knee |
| cerebral cortex (cloak) |
BRACHIAL BONE
If you take your hand back and bend it at the elbow, then at the top under the acromion, covered with a mouse. the upper rounded end of the humerus protrudes, and its two protrusions are clearly outlined at the bottom at the lower end (Fig. 18). The humerus lies among the mouse shoulder in the direction from top to bottom and somewhat from front to back. At the upper end of the bone are distinguished head, covered with articular cartilage; the head articulates with the articular cavity of the scapula, forming shoulder joint. Two tubercles protrude below the head: on the outer side of the bone big tubercle, on the inside- small tubercle. From each of them a bone ridge stretches down: crest of the greater tubercle and crest of the lesser tubercle are the attachment points for muscles.
On the outer side of the bone, slightly above the middle, there is deltoid tuberosity- site of attachment of the deltoid muscle. At the bottom, the humerus becomes flatter and widens. On the inside, there is a protrusion on it, noticeable when the arm is bent and unbent at the elbow, - internal epicondyle. Outside there is also a ledge - external epicondyle, which is noticeable only when the arm is bent at the elbow; when the arm is extended, he hides in the depths, the so-called pits of beauty. Between the epicondyles are two articular surfaces. One is located inside, has the shape of a block and is called block- it articulates with the ulna; the other lies outwards, resembles a ball in shape, is called capitate eminence and articulates with the radius. Above them in front is a recess - coronal fossa, behind a deeper depression - cubital fossa.
BONES OF THE FOREARM
Elbow and radius. If we consider the forearm on the arm bent at the elbow and with the palm open up, then on the back of the forearm you can detect and feel along its entire length a bone that starts at the top with the so-called elbow and ends at the bottom with a small thickening (head) lying on the side of the little finger - this is the ulna. thumb another bone, which further upwards hides among the muscles, and at the top appears on the surface under the external condyle of the shoulder and rests against the capitate eminence of the shoulder, with which it articulates, is the radius. If you put your fingers on its upper horses and turn the hand with your palm back, then you can feel how this bone turns, making a rotational movement around the longitudinal axis. If you feel the entire forearm during this movement, you can feel that with this turn of the hand with the palm down, the entire bone turns along with the hand and lies obliquely and on top of the ulna - this movement is called pronation and this position of the forearm is the position of pronation. If after that you make the opposite movement - turn the hand with the palm up, then simultaneously with the brush the radius will turn and lie parallel to the ulna - this movement is called supination, and the position of the forearm and hand is the position of supination.
The ulna serves as the base of the forearm (Fig. 19). It has a body and two ends; the ulna is longer than the radius, narrow below, and much more massive at the top, its upper end resembles a wrench, it has olecranon(the so-called elbow), and lower, in front, coronoid process. Between them lies crescent cut, which is a cartilage-covered articular platform for articulation with the block of the humerus. side, with outer side, available lesser crescent notch- articular platform for articulation with the head of the radius Below the large notch, in front, lies the ulnar tuberosity, to which the tendon of the brachialis muscle is attached. From top to bottom, the ulna narrows, and below it forms a slight expansion - head ulna; on the side of the head there is an articular platform for articulation with the lower end of the radius, and on the other inner side there is a small styloid process.
Figure 19 Bones of the forearm. BUT - right radial (I) and ulnar (II) bones in supination B-,(II)- right ulna outside:
I- olecranon, t- large lunate notch (covered with cartilage), 3 - head of the radius - articular platform for articulation with humerus. 4- articular platform for articulation with the ulna.
6 - radial tuberosity. 6 - styloid process.
7 - articular platform for articulation with the wrist,
8 - styloid process. 9 - head of the ulna, articular platform for articulation with the beam. 10 - ulnar tuberosity. // - articular platform for articulation with the head of the beam. /7 - coronoid process
The radius at the upper end has a cylindrical head, on the lateral surface of which lies the articular platform for articulation with the small lunate notch of the ulna, and at the top there is a recess in the form of a ball segment covered with cartilage - this is the articular platform for articulation with the capitate eminence of the humerus.
Slightly below the head protrudes tuberosity of the radius- site of attachment of the tendon of the biceps brachii muscle. Below, the radius expands, and together with the ulna forms the lower bone base of the forearm, visible on the arm.
At the lower end of the radius lies an articular platform for articulation with the wrist, on the inside there is a small articular platform for articulation with the ulna, and from the outside down the styloid process protrudes, which can be easily felt under the skin in the so-called anatomical snuffbox (see muscles).
The ulna and radius are articulated with each other at the top and bottom by two joints; these joints are cylindrical and one action is simultaneously performed in them - the rotation of the radius around the ulna; movement is accompanied by a turn brushes and is called pronation when the radius crosses the ulna and turns the hand with the palm back, and supination, when the radius lies next to the ulna and turns the hand with the palm forward (Plate I, Fig. 20).
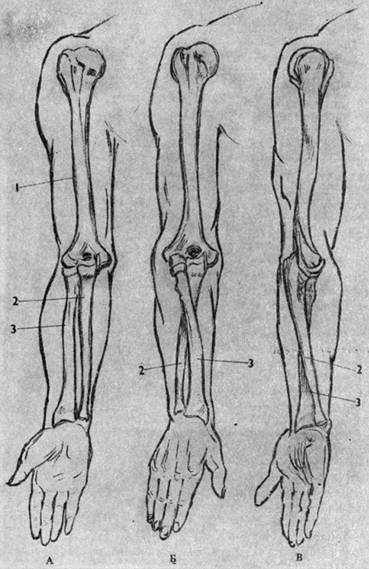
Rice. 20 Pronation of the forearm and shoulder (scheme): BUT- supination position; B- pronation of the forearm; AT- pronation of the forearm together with the pronation of the shoulder:
I- brachial bone. 2 - elbow bone. 3 - radius
At the top, the ulna articulates with the shoulder block joint, where flexion and extension movements occur; nearby, the radius also articulates with the shoulder, but with a spherical joint, in which flexion and extension movements occur (together with the ulna) and, in addition, rotational movements around the longitudinal axis of the radius during pronation or supination of the forearm. Pronation and supination of the forearm can occur both independently, when the elbow joint is immobile, and simultaneously with flexion and extension in the elbow joint (Table I).
The lower end of the radius carries the articular platform for articulation with the wrist. This platform is formed by the lower concave end of the radius and triangular cartilage fused with its inner edge, which protrudes between the lower end of the ulna and the wrist and separates them from each other. This cartilage is connected by a short ligament to the styloid process of the beam, and during pronation and supination, together with the lower end of the radius, rotates around this process. Thus, the wrist articulates only with the radius, the ulna does not participate in it, remaining only a support, and the wrist freely follows the radius during its rotation. This joint is called the wrist joint, in shape it is ovoid (ellipsoidal) - biaxial.
Check out the above on the model and on yourself. Build a hand with a shoulder blade at the back (the brush can not be depicted yet), draw the bones.
Questions. Shoulder blade and clavicle and their relief on the model. Joints of the shoulder girdle, jugular cavity. The concept of the shoulder girdle. Humerus, its relief on the model, shoulder joint. Ulna and radius bones, their relief on the model. elbow joint. The connection between the bones of the forearm. Pronation and supination of the arm.