Features of the structure and age-related changes in the musculoskeletal system. Anatomy, physiology of children with the basics of hygiene and physical education
The musculoskeletal system consists of bones, muscles, ligaments, tendons, cartilage, joints and joint capsules and is designed to ensure changes in body position and movement in space. Bones and their joints constitute the passive part of the musculoskeletal system, and muscles - its active part.
Musculoskeletal system in children
By the time the child is born, the ossification process is not completely completed. The diaphysis of tubular bones is represented by bone tissue, and the overwhelming majority of epiphyses, all cancellous bones of the hand and part of the tubular bones of the foot are made of cartilage. Ossification points in the pineal glands begin to appear only on last month intrauterine development and are planned for birth in the bodies and arches of the vertebrae, the epiphyses of the femurs and tibia, as well as the calcaneus, talus and cuboid bones. Ossification points in the epiphyses of the remaining bones appear after birth during the first 5-15 years, and the sequence of their appearance is quite constant. The totality of the ossification nuclei available in the child represents important characteristic the level of its biological development and is called "bone age".
Development skeletal system in children
After the birth of a child, bones grow rapidly, the musculoskeletal system develops. The growth of bones in length occurs due to the presence of epiphyseal cartilage (a small layer of cartilaginous tissue between the ossifying pineal gland and the diaphysis). The peripheral edge of this cartilage on the surface of the bone is called the epiphyseal line. The epiphyseal cartilage performs a bone-forming function until the bone reaches its final size (18-25 years). Subsequently, it is replaced by bone tissue and grows together with the pineal gland. Bone growth in thickness occurs due to the periosteum, in the inner layer of which young bone cells form a bone plate (periosteal method of bone formation).
The bone tissue of newborns has a porous, coarse-fiber mesh (bundle) structure. Bone plates are few and far between. Haversian channels appear to be disordered scattered cavities. The volumes of the intraosseous spaces are small and are formed with age. As the musculoskeletal system grows, multiple bone restructuring occurs, with the replacement of the fibrous mesh structure by the lamellar structure by the age of 3-4, with secondary Haversian structures.
Formation of the skeletal system in a child
The restructuring of bone tissue in children is more intensive. So, during the first year of life, 50-70% of the bone tissue is remodeled, and in adults during the year - only 5%.
By chemical composition the bone tissue of a child contains more water and organic matter and less minerals than that of adults. So, in newborns, ash is 1/2 of the bone mass, and in adults - 4/5. With age, the content of hydroxyapatite (its main mineral component) in bone increases. The fibrous structure and features of the chemical composition determine the greater elasticity of bones in children and their compliance with compression. Bones in children are less brittle, but bend and deform more easily.
The surfaces of the bones in children are relatively flat. Bony protrusions form as muscles develop and function actively.
The blood supply to bone tissue in children is more abundant than in adults, due to the number and large branching area of the diaphyseal, well-developed metaphyseal and epiphyseal arteries. By the age of 2, the child develops a single intraosseous circulatory system. Abundant vascularization provides intensive bone growth and rapid bone regeneration after fractures. At the same time, a rich blood supply with the presence of well-developed, perforating growth cartilage of epimetaphyseal vessels creates anatomical prerequisites for the occurrence of hematogenous osteomyelitis in children (up to 2-3 years of age, more often in the pineal glands, and at an older age - in the metaphyses). In children over 2 years of age, the number of blood vessels in the bones of the musculoskeletal system decreases significantly and increases again only by the time of prepubertal and pubertal growth acceleration.
Features of the development of the skeletal system in children
The periosteum in children is thicker than in adults, resulting in subperiosteal fractures of the "green line" type in the event of trauma. The functional activity of the periosteum in children is significantly higher than in adults, which ensures rapid transverse bone growth.
In prenatal period and in newborns, all bones are filled with red bone marrow, which contains blood cells and lymphoid elements and performs hematopoietic and protective functions. In adults, red bone marrow is contained only in the cells of the spongy substance of flat, short cancellous bones and the epiphyses of tubular bones. In the medullary cavity of the diaphysis of the tubular bones, there is a yellow bone marrow, which is a degenerated stroma with fatty inclusions. The most pronounced changes in bones occur during the first 2 years of life, in the younger school age and during puberty. Only by the age of 12, the bones of a child external structure and the histological features approach those of an adult.
Joint formation in children
Age features joints in children
By the time of birth, the articular-ligamentous apparatus is anatomically formed. Newborns already have all the anatomical elements of the joints, but the epiphyses of the articulating bones consist of cartilage.
The capsules of the joints of the newborn are tightly stretched, and most of the ligaments are characterized by insufficient differentiation of the fibers that form them, which determines their greater extensibility and lower strength than in adults. These features determine the possibility of subluxation, for example, the head of the radius and humerus.
Joint development occurs most intensively before the age of 3 years and is due to a significant increase in motor activity child. Over the period from 3 to 8 years in children, the range of motion in the joints gradually increases, the process of restructuring of the fibrous membrane of the articular capsule and ligaments is actively continuing, and their strength increases. At the age of 6-10 years, the structure of the articular capsule becomes more complicated, the number of villi and folds of the synovial membrane increases, vascular networks and nerve endings of the synovial membrane are formed. At the age of 9-14 years, the process of restructuring of the articular cartilage slows down. The formation of articular surfaces, capsules and ligaments is mainly completed only by 13-16 years of age.
Send your good work in the knowledge base is simple. Use the form below
Students, graduate students, young scientists who use the knowledge base in their studies and work will be very grateful to you.
Posted on http://www.allbest.ru/
Karaganda State Medical University
Department of Normal Physiology
CDS on the topic:
Age physiology musculoskeletal system in children
Is done by a student
Blum Evgeniy 3-094 ОМ
Checked by: Meyramova A.G.
Karaganda 2013
Introduction
1. Anatomical and physiological features of the musculoskeletal system
2. Age features of joints in children
3. Anatomical and physiological features of the muscular system
Introduction
With age, the content of hydroxyapatite (its main mineral component) in bone increases. The fibrous structure and features of the chemical composition determine the greater elasticity of bones in children and their compliance with compression. Bones in children are less brittle, but bend and deform more easily.
The surfaces of the bones in children are relatively flat. Bony protrusions form as muscles develop and function actively.
The blood supply to bone tissue in children is more abundant than in adults, due to the number and large branching area of the diaphyseal, well-developed metaphyseal and epiphyseal arteries. By the age of 2, the child develops a single intraosseous circulatory system. Abundant vascularization provides intensive bone growth and rapid bone regeneration after fractures. The peripheral edge of this cartilage on the surface of the bone is called the epiphyseal line. The epiphyseal cartilage performs a bone-forming function until the bone reaches its final size (18-25 years). Subsequently, it is replaced by bone tissue and grows together with the pineal gland. Bone growth in thickness occurs due to the periosteum, in the inner layer of that young bone cells form a bone plate (periosteal method of bone formation).
The bone tissue of newborns has a porous, coarse-fiber mesh (bundle) structure. Bone plates are few and far between. Haversian channels appear to be disordered scattered cavities. The volumes of the intraosseous spaces are small and are formed with age. As it grows, there is a repeated restructuring of the bone, with the replacement of the fibrous mesh structure by the lamellar structure by the age of 3-4 years, with secondary Haversian structures.
The restructuring of bone tissue in children is more intensive. So, during the first year of life, 50-70% of the bone tissue is remodeled, and in adults during the year - only 5%.
In terms of chemical composition, the bone tissue of a child contains more water and organic matter and less minerals than that of adults. So, in newborns, ash is 1/2 of the bone mass, and in adults - 4/5. The musculoskeletal system consists of bones, muscles, ligaments, tendons, cartilage, joints and joint capsules and is designed to ensure changes in body position and movement in space. Bones and their joints constitute the passive part of the musculoskeletal system, and muscles - its active part.
1. Anatomical and physiological features of the musculoskeletal system
PeculiaritiesTorestWithsystems
The skeletal system in children is characterized by a number of features.
By the time the child is born, the ossification process is not completely completed. The diaphysis of tubular bones is represented by bone tissue, and the overwhelming majority of epiphyses, all cancellous bones of the hand and part of the tubular bones of the foot are made of cartilage. Ossification points in the epiphyses begin to appear only in the last month of intrauterine development and are outlined by birth in the bodies and arches of the vertebrae, the epiphyses of the femurs and tibia, as well as the calcaneus, talus and cuboid bones. Ossification points in the epiphyses of the remaining bones appear after birth during the first 5-15 years, and the sequence of their appearance is quite constant. The totality of ossification nuclei available in a child is an important characteristic of the level of his biological development and is called "bone age".
After the birth of a child, bones grow rapidly. The growth of bones in length occurs due to the presence of epiphyseal cartilage (a small layer of cartilaginous tissue between the ossifying pineal gland and the diaphysis). At the same time, a rich blood supply with the presence of well-developed, perforating growth cartilage of epimetaphyseal vessels creates anatomical prerequisites for the occurrence of hematogenous osteomyelitis in children (up to 2-3 years of age, more often in the pineal glands, and at an older age - in the metaphyses). In children over 2 years of age, the number of blood vessels in the bones decreases significantly and increases again only by the time of prepubertal and pubertal growth acceleration.
The periosteum in children is thicker than in adults, resulting in subperiosteal fractures of the "green line" type in the event of trauma. The functional activity of the periosteum in children is significantly higher than in adults, which ensures rapid transverse bone growth.
In the prenatal period and in newborns, all bones are filled with red bone marrow, which contains blood cells and lymphoid elements and performs hematopoietic and protective functions. In adults, red bone marrow is contained only in the cells of the spongy substance of flat, short cancellous bones and the epiphyses of tubular bones. In the medullary cavity of the diaphysis of the tubular bones, there is a yellow bone marrow, which is a degenerated stroma with fatty inclusions. The most pronounced changes in bones occur during the first 2 years of life, during primary school age and during puberty. Only by the age of 12, the bones of a child in their external structure and histological features approach those of an adult.
2. Age features of joints in children
By the time of birth, the articular-ligamentous apparatus is anatomically formed. Newborns already have all the anatomical elements of the joints, but the epiphyses of the articulating bones consist of cartilage.
The capsules of the joints of the newborn are tightly stretched, and most of the ligaments are characterized by insufficient differentiation of the fibers that form them, which determines their greater extensibility and lower strength than in adults. These features determine the possibility of subluxation, for example, of the head of the radius and humerus.
Joint development occurs most intensively before the age of 3 years and is due to a significant increase in the child's motor activity. Over the period from 3 to 8 years in children, the range of motion in the joints gradually increases, the process of restructuring of the fibrous membrane of the articular capsule and ligaments is actively continuing, and their strength increases. At the age of 6-10 years, the structure of the articular capsule becomes more complicated, the number of villi and folds of the synovial membrane increases, vascular networks and nerve endings of the synovial membrane are formed. At the age of 9-14 years, the process of restructuring of the articular cartilage slows down. The formation of articular surfaces, capsules and ligaments is mainly completed only by 13-16 years of age.
Scull
The skull at the time of birth is represented by a large number of bones connected by wide cartilaginous and connective tissue layers. Thickening and pneumatization of the bones occurs, which leads to a decrease in their mass.
Spine
Length spinal column in a newborn it is 40% of its body length and doubles in the first 2 years of life. However, different parts of the spinal column grow unevenly, for example, in the first year of life, the lumbar region grows most rapidly, and the coccygeal region grows slowest.
In newborns, the vertebral bodies, as well as the transverse and spinous processes, are relatively poorly developed, the intervertebral discs are relatively thicker than in adults, they are better supplied with blood.
The spine of a newborn has the form of a gentle arc, concave in front. Physiological curves begin to form only from 3-4 months. Cervical lordosis develops after the child begins to hold his head. The seams between the bones of the fornix (sagittal, coronal, occipital) are not formed and begin to close only from the 3rd-4th month of life. The edges of the bones are even, the teeth are formed only in the 3rd year of the child's life. The formation of sutures between the bones of the skull ends by 3-5 years of age. The overgrowth of seams begins after 20-30 years.
Most characteristic feature skull of a newborn - the presence of fontanelles (non-ossified membranous areas of the cranial vault), due to which the skull is very elastic, its shape can change during the passage of the fetal head through the birth canal (Fig. 2-10).
The large fontanelle is located at the intersection of the coronal and sagittal sutures. Its dimensions are from 1.5x2 cm to 3x3 cm when measured between the edges of the bones. The large fontanelle closes usually by the age of 1-1.5 years (nowadays, it is often already by the 9-10th month of life).
The small fontanelle is located between the occipital and parietal bones; by the time of birth, it is closed in 3/4 of healthy full-term babies, and in the rest it closes by the end of 1–2 months of life.
Lateral fontanelles (anterior wedge-shaped and posterior mastoid) in term infants are closed at birth.
The cerebral section of the skull is significantly larger in volume than the facial one (in a newborn, it is 8 times, and in adults only 2 times). The newborn's eye sockets are wide, the frontal bone consists of two halves, the superciliary arches are not pronounced, the frontal sinus is not formed. The jaws are underdeveloped, the lower jaw consists of two halves.
The skull grows rapidly up to 7 years. In the first year of life, there is a rapid and uniform increase in the size of the skull, the thickness of the bones increases by 3 times, the structure of the bones of the cranial vault is formed. At the age of 1 to 3 years, ossification points merge, cartilaginous tissue is gradually replaced by bone. On the 1-2nd year, halves grow together lower jaw, in the 2-3rd year, due to the strengthening of the function of the chewing muscles and the completion of the eruption of milk teeth, the growth of the facial skull increases. From 3 to 7 years of age, the base of the skull grows most actively, and by the age of 7 years its growth in length basically ends. At the age of 7-13, the skull grows more slowly and evenly. At this time, the fusion of individual parts of the skull bones is completed. At the age of 13-20 years, mainly the facial part of the skull grows, sex differences appear. The acetabulum in a newborn is oval, its depth is much shallower than in an adult, as a result of which most of the head femur located outside of it. The articular capsule is thin, the ischio-femoral ligament is not formed. Gradually, with the growth of the pelvic bone in thickness and the formation of the edge of the acetabulum, the head of the femur sinks deeper into the joint cavity.
Limbs
In newborns, the limbs are relatively short. Subsequently, the lower limbs grow faster and become longer than the upper ones. Fastest growth rate lower limbs occurs in boys aged 12-15 years, in girls aged 13-14 years.
In a newborn and a baby in the first year of life, the foot is flat. When the child begins to sit (5-6 months), thoracic kyphosis appears. Lumbar lordosis begins to form after 6-7 months, when the child begins to sit, and intensifies after 9-12 months, when the child begins to stand and walk. At the same time, sacral kyphosis is formed compensatory. The bends of the spinal column become clearly visible by the age of 5-6 years. The final formation of cervical lordosis and thoracic kyphosis is completed by the age of 7 years, and lumbar lordosis - by the period of puberty. Thanks to the bends, the elasticity of the spinal column increases, shocks and concussions when walking, jumping, etc. are softened.
Due to the incompleteness of the formation of the spine and the poor development of muscles that fix the spine, children easily develop pathological bends of the spine (for example, scoliosis) and posture disorders.
Rib cage
The chest of a newborn has a conical shape, its anteroposterior size is larger than the transverse one. The ribs extend from the spine almost at right angles, and are located horizontally. The rib cage is, as it were, in the position of maximum inspiration.
Ribs in children early age soft, pliable, easy to bend and springy when pressed. The depth of inspiration is provided mainly by the excursions of the diaphragm, the place of attachment of the diaphragm, when breathing is difficult, is retracted, forming a temporary or permanent Harrison groove.
As the baby begins to walk, the sternum drops and the ribs gradually take on a tilted position. By the age of 3 years, the anteroposterior and transverse dimensions of the chest are equal in size, the angle of inclination of the ribs increases, and costal breathing becomes effective. anatomical physiological bone muscle child
By school age, the chest flattens, depending on the type of physique, one of its three forms begins to form: conical, flat or cylindrical. By the age of 12, the chest moves to the maximum expiratory position. Only by the age of 17-20 does the chest take on its final shape.
Pelvic bones
The pelvic bones in young children are relatively small. The shape of the pelvis resembles a funnel. The pelvic bones grow most intensively during the first 6 years, and in girls, in addition, in puberty... The change in the shape and size of the pelvis occurs under the influence of body weight, organs abdominal cavity, under the influence of muscles and the influence of sex hormones. The difference in the shape of the pelvis in boys and girls becomes noticeable after 9 years: in boys, the pelvis is taller and narrower than in girls.
Up to 12-14 years old, the pelvic bone consists of 3 separate bones connected by cartilage, the fused bodies of which form the acetabulum. The line of the transverse joint of the tarsus is almost straight (in an adult it is S-shaped). The formation of the articular surfaces, ligaments and arches of the foot occurs gradually, after the child begins to stand and walk and as the bones of the foot ossify.
Teeth
Milk teeth in children usually erupt from the age of 5-7 months in a certain sequence, while the teeth of the same name on the right and left halves of the jaw appear simultaneously. The order of eruption of milk teeth is as follows: 2 internal lower and 2 internal upper incisors, and then 2 external upper and 2 external lower incisors (by the year - 8 incisors), at the age of 12-15 months. - anterior molars (molars), at 18-20 months. - canines, at 22-24 months. - posterior molars. Thus, by the age of 2, a child has 20 milk teeth. For an approximate determination of the proper number of milk teeth, you can use the following formula:
where: X is the number of milk teeth;
n is the child's age in months.
The period of replacing milk teeth with permanent ones is called the period of a changeable bite. Permanent tooth usually erupts after 3-4 months. after the loss of milk. The formation of both milk and permanent bite in children is a criterion for the biological maturation of a child (dental age).
In the first period (from eruption to 3-3.5 years), the teeth stand closely, the bite is orthognathic (the upper teeth cover the lower ones by one third) due to underdevelopment the lower jaw, there is no wear of the teeth.
In the second period (from 3 to 6 years), the bite becomes straight, physiological gaps appear between milk teeth (as preparation for the eruption of permanent, wider teeth) and their wear.
The change of milk teeth to permanent ones begins at the age of 5. The order of eruption of permanent teeth is usually the following: at 5-7 years old the first molars (large molars) erupt, at 7-8 years old - internal incisors, at 8-9 years old - external incisors, at 10-11 years old - anterior premolars , at 11-12 years old - posterior premolars and canines, at 10-14 years old second molars, at 18-25 years old - wisdom teeth (may be absent). For a rough estimate of the number of permanent teeth, you can use the formula:
where: X is the number of permanent teeth,
n is the child's age in years.
In some children, teething may be accompanied by an increase in body temperature, sleep disturbances, diarrhea, etc. The formation of both milk and permanent bite in children - important indicator biological maturation of the child. A permanent bite should normally be orthognathic or straight.
Along with the development of muscle fibers, endomysium and perimisia are formed. The muscular system includes more than 600 muscles, most of which are involved in various movements.
3. Anatomical and physiological features of the muscular system
By the time of birth, the number of muscles in a child is almost the same as in an adult, but there are significant differences in terms of mass, size, structure, biochemistry, physiology of muscles and neuromuscular units.
Skeletal muscles in a newborn are anatomically formed and relatively well developed, their total mass is 20-22% of body weight. By the age of 2, the relative muscle mass decreases slightly (up to 16.6%), and then, due to the increase in the child's motor activity, it increases again and by the age of 6 it reaches 21.7%, by 8-27-28%, and by 15-32 -33%. In adults, it averages 40-44% of body weight. In total, muscle mass increases 37 times during childhood.
The structure of skeletal muscle tissue in children different ages has a number of differences. In a newborn, muscle fibers are located loosely, their thickness is 4-22 microns. Postnatal growth muscle mass occurs mainly due to the thickening of muscle fibers, and by the age of 18-20 their diameter reaches 20-90 microns. In general, the muscles in young children are thinner and weaker, and the muscle relief is smoothed out and usually becomes distinct only by 5-7 years of age.
The fascia of a newborn is thin, loose, easily detached from the muscles. So, the weak development of the tendon helmet and its loose connection with the periosteum of the bones of the cranial vault predispose to the formation of hematomas when the child passes through the birth canal. The maturation of the fascia begins from the first months of a child's life and is associated with the functional activity of the muscles. There is relatively much interstitial tissue in the muscles of a newborn. In the first years of life, there is an absolute increase in loose intramuscular connective tissue, and the relative number of cellular elements per unit area decreases. Its differentiation ends by the age of 8-10.
The nervous apparatus of muscles at the time of birth is not fully formed, which is combined with the immaturity of the contractile apparatus of skeletal muscles. As the child grows, both the motor innervation of the phasic skeletal muscle fibers mature (change from polyneuronal to mononeural innervation, a decrease in the area of sensitivity to acetylcholine, in mature neuromuscular synapses confined only to the postsynaptic membrane) and the formation of definitive neuromuscular units. There is also the formation of new proprioceptors with their concentration in the muscle areas experiencing the greatest stretching.
Skeletal muscles in newborns are characterized by a lower content of contractile proteins (in newborns they are 2 times less than in older children), the presence of a fetal form of myosin, which has a small ATPase activity. As the child grows, fetal myosin is replaced by definitive myosins, the content of tropomyosin and sarcoplasmic proteins increases, and the amount of glycogen, lactic acid and water decreases.
A child's muscles are characterized by a number of functional features. So, children celebrate increased sensitivity muscles to some humoral agents (in particular, to acetylcholine). In the prenatal period, skeletal muscles are characterized by low excitability. The muscle reproduces only 3-4 contractions per second. With age, the number of contractions reaches 60-80 per second. Maturation of the neuromuscular synapse leads to a significant acceleration of the transition of excitation from the nerve to the muscle. In newborns, the muscles do not relax, not only during wakefulness, but also during sleep. Their constant activity is explained by the participation of muscles in heat production (the so-called contractile thermogenesis) and metabolic processes of the body, stimulating the development of muscle tissue itself. Muscle tone can be a guideline when determining gestational age newborn. So, in healthy children, the first 2-3 months. life celebrate increased tone flexor muscles, the so-called physiological hypertonicity, associated with the peculiarities of the functioning of the central nervous system and leading to some limitation of mobility in the joints. Hypertonia in the upper extremities disappears in 2-2.5 months, and in the lower ones - in 3-4 months. Deep premature babies(gestational age less than 30 weeks) are born with general muscle hypotension. In a child born at 30-34 weeks of gestation, the lower limbs are bent at the hip and knee joints... Flexion upper limbs appears only in children born after the 34th week of gestation. After the 36-38th week, the flexor position of both the lower and upper limbs is noted.
The growth and development of muscles in children is uneven and depends on their functional activity. So, in a newborn, mimic and chewing muscles are poorly developed. They are noticeably strengthened after the eruption of milk teeth. Age-related features of the diaphragm are clearly expressed. Its dome in newborns is more convex, the tendon center occupies a relatively small area. As the lungs develop, the bulge of the diaphragm decreases. In children under 5 years of age, the diaphragm is located high, which is associated with the horizontal course of the ribs.
In newborns, the muscles, aponeuroses and fascia of the abdomen are poorly developed, which determines the convex shape of the anterior abdominal wall, which lasts up to 3-5 years. The umbilical ring in a newborn is not yet formed, especially in its upper part, in connection with which the formation of umbilical hernia... Insufficient muscle development occurs in children leading a sedentary lifestyle, with dystrophy caused by malnutrition, the presence of chronic somatic diseases, pathology nervous system, generalized joint damage, etc.
The extreme degree of poor muscle development is atrophy. In this condition, the mass of muscle tissue is sharply reduced, and the abdomen of the muscles in its thickness and consistency becomes similar to a tendon. With muscle atrophy, a reversible or irreversible violation of muscle trophism occurs with the development of thinning and degeneration of muscle fibers, weakening or loss of their contractility. The asymmetry of muscle mass suggests an unequal degree of development of the muscle groups of the same name. To identify asymmetry, similar muscles of both halves of the face, trunk, and limbs are consistently compared. For a more accurate assessment, measure with a measuring tape and compare the circumferences of the left and right limbs at the same levels.
Muscular asymmetry can be the result of underdevelopment, trauma, pathology of the nervous system, some rheumatic diseases (hemiscleroderma, JRA), etc.
Palpation reveals local or widespread soreness, as well as compaction along the muscles, which may be associated with inflammatory changes, focal or diffuse deposition of calcium in them.
Muscle tone
Muscle tone is a reflex muscle tension controlled by the central nervous system and also dependent on metabolic processes occurring in the muscle. Decrease or absence of tone is called hypotension or muscle atony, respectively, normal tone- muscle normotonia, high tone- muscle hypertension.
A preliminary idea of the state of muscle tone can be obtained from a visual assessment of the posture and position of the child's limbs. So, for example, the pose of a healthy newborn (arms bent at the elbows, knees and hips pulled up to the stomach) indicates the presence of physiological hypertonicity of the flexors. With a decrease in muscle tone, the newborn lies on the table with outstretched arms and feet. In older children, a decrease in muscle tone leads to postural disorders, pterygoid scapula, excessive lumbar lordosis, abdominal enlargement, etc.
Muscle tone is examined by assessing the muscle resistance that occurs during passive movements in the corresponding joints (the limb should be as relaxed as possible).
Toning can be of two types.
-- muscular spasticity - resistance to movement is expressed only at the beginning of passive flexion and extension, then the obstacle seems to decrease (the "folding knife" phenomenon). It occurs when the central influence on the cells of the anterior horn of the spinal cord is interrupted and the segmental reflex apparatus is disinhibited.
-- muscular rigidity - hypertonicity is constant or increases with repetition of movements (the phenomenon of “ wax doll"Or" lead tube "). In the study of muscle tone, intermittency, stepped resistance (the phenomenon of "cogwheel") may occur. The limb can freeze in the position that is given to it - plastic tone. It occurs when the extrapyramidal system is damaged.
With muscular hypotension, there is no resistance during passive movements, a flabby muscle consistency, an increase in volume
joint movements (for example, overextension). There are several tests to judge the state of muscle tone in children.
A symptom of return - the legs of a newborn, lying on his back, are unbent, straightened and pressed to the table for 5 seconds, after which they are released. So, the dynamometry indicators in boys are higher than in girls. The exception is the period from 10 to 12 years old, when the strength of the girls is higher than that of boys. The relative strength of muscles (per 1 kg of body weight) changes insignificantly up to 6-7 years old, and then increases rapidly by the age of 13-14 years. Muscle endurance also increases with age, and in 17-year-olds it is twice as high as in 7-year-olds.
Muscle development
In healthy children, muscles are elastic to the touch, the same on symmetrical parts of the body and limbs. There are 3 degrees of muscle development.
Good - the contours of the muscles of the trunk and limbs at rest are clearly visible, the stomach is pulled in or slightly protrudes forward, the shoulder blades are pulled up to the chest, the relief of the contracted muscles increases with tension.
Average - the muscles of the trunk are moderately developed, and the limbs are well developed, with tension, their shape and volume clearly change.
Weak - at rest, the muscles of the trunk and limbs are poorly contoured, with tension, the relief of the muscles changes barely noticeably, Bottom part the abdomen sags, the lower angles of the shoulder blades diverge and lag behind the chest. The superficial inguinal ring forms a funnel-shaped protrusion, more pronounced in girls.
In a newborn, the mass of the muscles of the trunk predominates. In the first years of a child's life, due to an increase in motor activity, the muscles of the extremities grow rapidly, and the development of the muscles of the upper extremities at all stages outstrips the development of the muscles of the lower extremities. First of all, the large muscles of the shoulder, forearm develop, much later, the muscles of the hand, which leads to difficulties in performing thin self made up to 5-6 years of age. Until the age of 7, children have insufficiently developed leg muscles, and therefore they do not tolerate long-term loads poorly. At the age of 2-4 years, the gluteus maximus muscles and the long back muscles grow vigorously. The muscles that ensure the vertical position of the body grow most intensively after 7 years, especially in adolescents 12-16 years old. Improvement of accuracy and coordination of movements most intensively occurs after 10 years, and the ability to move quickly develops only by 14 years.
The intensity of muscle gain and muscle strength is gender-related. If a newborn has physiological hypertonicity, the legs immediately return to their original position, with a reduced tone, a complete return does not occur.
Traction test - a child lying on his back is taken by the wrists and tried to be transferred to a sitting position. The child first unbends his arms (first phase), and then bends them, pulling his whole body towards the investigator (second phase). With hypertonicity, the first phase is absent, and with hypotonia - the second phase.
Symptom of the "rope" - the researcher, standing facing the child, takes him in his hands and makes rotational movements alternately in one direction or the other, while assessing the degree of active muscle resistance.
A symptom of "flabby shoulders" - the shoulders of the child are wrapped around the back with two hands and actively lifted up. With hypotonia, this movement is easy, with the shoulders touching the earlobes.
Range of motion
The volume of both active and passive movements is assessed.
Active movements are studied in the process of observing the child while playing, walking, performing certain movements (squatting, bending, raising arms and legs, stepping over obstacles, climbing and descending stairs, etc.). The limitation or absence of movements in certain muscle groups and joints indicates damage to the nervous system (paresis or paralysis), muscles, bones, joints.
Passive movements are examined by sequentially flexing and extending the joints: elbow, hip, ankle, etc. In newborns and children of the first 3-4 months of life, limitation of movements in the joints is noted, due to physiological hypertonicity. Restriction of passive movement in older children indicates increased muscle tone or joint damage.
Muscle strength
Muscle strength is assessed by the degree of effort required to overcome the active resistance of a particular muscle subgroup. They try to take away the toy they seized from young children. Older children are asked to provide resistance when extending the bent arm (leg). The state of muscle strength can be indirectly judged by how the child performs squats, going up and down stairs, getting up from the floor or bed, dressing and undressing, etc. muscular strength clearly increases with age. As a rule, the dominant hand is stronger, and in general muscular boys have more strength than girls. More objectively, you can judge muscle strength by the displays of the dynamometer (hand and back).
Laboratory and instrumental research
For diseases of the muscular system, examine biochemical parameters blood [activity of creatine phosphokinase, muscle fraction of lactate dehydrogenase (LDH), transaminases, concentration of amino acids and creatine in blood and urine, myoglobin content in blood and urine], determine autoantibodies. To clarify the diagnosis, genetic and morphological studies of muscle biopsy are performed.
Among the instrumental methods for elucidating the cause of a decrease in muscle strength in clinical practice, electromyography (EMG) is most often used - a method of recording the bioelectric activity of muscles, which, for example, makes it possible to differentiate the primary pathology of muscles from their lesions in diseases of the nervous system. Muscle excitability is assessed using chronaximetry, muscle performance - with an ergograph and an ergometer.
Bibliography:
1. Fundamentals of Human Physiology / Under. ed. ON THE. Aghajanyan. - M .: RUDN, 2001
2. Human physiology / Under. ed. V.M. Pokrovsky, G.F. Shortly. - M .: Medicine, 2003
3. Physiology of the fetus and children / Under. ed. V.D. Glebovsky - M .: Medicine, 1988.
Posted on Allbest.ru
...Similar documents
general characteristics and age-related features of cartilage tissue. Types of cartilage and bone tissue. General characteristics and age characteristics of bone tissue. Features of the structure of muscle tissue in childhood and old age. Skeletal muscle tissue.
presentation added 02/07/2016
Anatomical and physiological features of the respiratory system, blood circulation in children. Cardiovascular, urinary and nervous systems. Analysis of the development of the musculoskeletal system in childhood... Functions digestive system and blood systems.
presentation added on 12/28/2014
General characteristics of the motor activity of animals. Acquaintance with the structure of the system of tissues and organs - the musculoskeletal system. Description of the main functions of the skeleton of an animal. Study of the peculiarities of the neuromuscular part of the motor apparatus.
abstract added 10/26/2015
Study of the structure and characteristics of the elements of the human musculoskeletal system as a functional set of skeletal bones, tendons and joints that provide motor actions. The functions of the locomotor system: support, protective, spring.
test, added 01/06/2011
System of organs of movement: bones (skeleton), ligaments, joints and muscles. Characterization of bone tissue, consisting of cells and intercellular substance. Three periods of development of the skull after birth. Age features of the spine and skeletal muscles.
abstract, added 06/06/2011
Anatomical and physiological features of the nervous system in newborns. Functional features nervous system in children. Psychomotor development children. Unconditioned, visceral and autonomic reflexes of newborns. Age-related histological features.
term paper added 05/17/2015
Periods of dental development in children. Morphological features of the intrauterine period. Time from birth to the beginning of the eruption of deciduous teeth, the period of formation of their bite. Formed milk and replaceable bites. Period of occlusion of permanent teeth.
presentation added on 12/16/2015
Voluntary and involuntary muscles. Abduction and inward rotation are the main functions of the muscles. Properties of muscle tissue: excitability, contractility, extensibility, elasticity. Function of skeletal (somatic) muscles. Features of the muscles of synergists and antagonists.
presentation added on 12/13/2010
The histological structure of the respiratory part of the lungs. Age-related changes and anatomical and physiological features of the respiratory part of the lungs. Research features respiratory system in children. The composition of the alveolar epithelium. Bronchial tree.
presentation added on 10/05/2016
Laying of the respiratory system in the human embryo. Anatomical and physiological features of the respiratory system in young children. Palpation of the patient during the examination of the respiratory system, percussion and auscultation of the lungs. Evaluation of spirographic indicators.
The human skeleton is about tissue - 15% of body weight. Bone is the densest connective tissue. Macroscopically, two types of skeletal bones are distinguished: flat and tubular.
Outside bones (cortical or compact) makes up about 70% of the bone tissue of the skeleton. The compact substance is part of the flat bones, the diaphysis of the long bones and covers all the bones from the outside in a thin layer.
Inner part (trabecular, or spongy) consists of calcified trabeculae filled with bone marrow, presented at the ends of tubular bones, between two layers of compact substance in the flat bones of the skull, scapula, sternum, ribs. This bone structure ensures optimal mechanical function with minimal bone mass. The microscopic structure of the cortical and cancellous bones is different.
In the cortical bone, the tissue consists of osteons, in the center of which there is a channel with blood vessels; osteons are separated from each other by cement lines. The cancellous bone is composed of structural units (packages), which are also separated from each other by cement lines, but they do not have blood vessels and it is nourished from the surface.
Outside, the bone is covered with periosteum, a thin connective tissue sheath containing blood vessels and nerves. In bone tissue, osteoblasts and osteoclasts are distinguished. Osteoblasts synthesize collagen fibers and matrix. After bone mineralization, osteoblasts turn into osteocytes. Osteoclasts are able to resorb calcified cartilage and intercellular substance of bone tissue in the process of bone development and remodeling.
Throughout life, bone tissue is constantly rebuilt. when the processes of destruction of the old and the formation of new bone are balanced (remodeling). In an adult, 25% of the cancellous bone and about 3% of the cortical bone are renewed annually. Remodeling begins in the womb and continues throughout life. Bone remodeling is closely related to calcium-phosphorus metabolism and is regulated by a complex hormonal system, in which the parathyroid hormone of the parathyroid glands, calcitonin of the thyroid gland and vitamin D play a leading role.
Slow bone loss occurs in men and in premenopausal women. After menopause, bone loss in women accelerates significantly. Bone tissue in the musculoskeletal system ensures the movement of the body in space and protects vital organs. The elements necessary for the vital activity of the body are deposited in the bone tissue, including about 99% of all calcium, 87% of phosphorus, 50% of magnesium, 46% of sodium, between the blood and bone tissue there is a constant exchange of calcium and phosphorus. The metabolic function of the bone is carried out by stabilizing the acid-base state.
With age in the musculoskeletal system as a result of stresses during life and age decline neuromuscular influences, degenerative-destructive changes occur. With aging, the volume of muscle mass decreases, the contractility of the muscles worsens, the number of functioning capillaries decreases, the muscles become atrophic and flabby. In muscle cells, there is an increase in fat inclusions and lipofuscin.
Bones are reduced in mineral content, there is a decrease in bone mass, they become less durable.
By the age of 60, pronounced changes in the spine are observed in almost all people. From the age of 50, senile growth begins to decrease due to a decrease in the height of the vertebral bodies and intervertebral discs.
The musculoskeletal system consists of the skeleton (bones), muscles, ligaments and joints. These structures form cavities for internal organs, protect internal organs, and also provide motor acts.
The skeleton (Fig, 24) forms the structural basis of the body, determines its shape and size. In the skeleton of an adult, there are more than 200 bones, which primarily perform a supporting function and are a kind of levers in the implementation of motor acts. Along with this, bones are actively involved in metabolic processes: they accumulate mineral salts and, if necessary, supply them to the body (mainly calcium and phosphorus salts). Bones also contain hematopoietic tissue - red bone marrow.
Bones contain approximately 60% minerals, 30% organic components (mainly ossein protein and osteoblastic bone cell bodies) and 10% water. Such a combination of substances in the structure of bones provides them with significant strength (30 times stronger than brick and 2.5 times stronger than granite) and greater elasticity, elasticity and viscosity (9 times higher than the viscosity of lead). The bones are characterized by a significant safety margin (for example, the femur can withstand a load of 1.5 tons). In children, tubular bones grow in length due to the cartilage between the ends of the bones (pineal glands) and their body (diaphysis), and in thickness - due to the surface tissue - the periosteum. Flat bones grow in all directions
only due to the periosteum. At the time of the end of the growth of the human body, the cartilage in many bones is replaced by bone tissue. The development of the skeleton in men ends at 20-24 years, and in women - at 17-21 years.
Separate bones and. even parts of the skeleton mature in different periods... So, up to 14 years old, only the middle parts of the vertebrae are covered by ossification, while their other parts remain cartilaginous and only at 21-23 years they completely become bony. By the same period, the ossification of most other bones of the skeleton is basically completed.
An important stage in the development of the human skeleton is the formation and consolidation of the bends of the spine (Fig. 25), which are divided into those that are directed with the convex side forward and are called lordosis (occur in the neck and lumbar spine) and those that are directed backwards and are called kyphosis (thoracic and sacral spine). Availability

lordosis and kyphosis is a necessary phenomenon due to the erect posture of a person when standing and walking; it is also required to maintain balance of the body and provide the function of shock absorption when moving, jumping, etc. Sagittal (when viewed from the side) bends of the spine appear from the moment when children begin to raise their heads, sit down, get up and walk (at the age of up to one year). Up to 5-6 years of age, the folds of the spine are not very fixed, and if the child lies down, then most often these folds disappear (align). Fastening of the bends of the spine occurs gradually: until 7-8 years old, only the cervical and thoracic bends are formed, and at 12-14 years old - lordosis of the lumbar spine and kyphosis of the sacral spine. The final consolidation of lordosis and kyphosis is completed with ossification of the vertebrae of the spine (17-20 years). In frontal projection (when viewed from the front or rear), the normally developed spine should be straight.
Deviations from the normal shape of the spine can be: a straightened spine, when lordosis and kyphosis are insufficiently developed due to reasons, for example, little child's mobility; lordotic or kyphatic spine, when lordosis or kyphosis is increased, respectively. Bends of the spine to the left or to the right determine the scoliotic shape of the spine. The spine shapes create the corresponding body posture (posture) shapes: normal, erect, lordotic, kyphatic (stooped) or scoliotic.
Together with the formation of the spine in children, the chest also develops, which acquires a normal cylindrical shape, like in adults, at about 12-13 years old, and then it can increase up to 25-30 years only in size. Deviations in the development of the shape of the chest are most often: a conical shape (narrowed up) and a flattened shape (reduced front-wheel drive rear dimensions). Various deviations from the development of normal forms of the spine and chest can negatively affect not only the posture of the body, but also disrupt the normal development of internal organs, and worsen the level of somatic health.
Deviations in the shape of the spine and chest in children can be caused by improper sitting at a desk or table (bending to the side, low bends over the desk or lagoon on the edge of the table, etc.), Incorrect posture when standing and walking (lowering one shoulder below the other, lowering head, stoop), physical overload, especially lifting and carrying heavy things, including in one hand. For the prevention and prevention of deviations in the development of the skeleton of the trunk, it is necessary to observe hygiene requirements work at the table (desk) and exercise hygiene. The normal development of the spine and chest is greatly facilitated by rational physical exercise... Specialized physical exercise can also be one of the most effective measures to eliminate deviations in the development of the skeleton, including stoop, scoliosis, etc.
The skeleton of the upper limbs consists of the shoulder girdle of the upper limbs, including two shoulder blades and two clavicles, and the skeleton of the free upper limb. The latter, in turn, consists of humerus, bones in front of the shoulder (ulna and radius) and bones of the hand (8th bones of the zap "yast, 5th bones of the n" yast and bones of the phalanges of the fingers: thumb - 2, the rest of the fingers - 3 phalanges).
The skeleton of the lower limbs is made up of bones pelvic girdle and bones of the free lower limb. The pelvic girdle, in turn, is formed by the sacral bone (five sacral vertebrae, grow together), the tailbone and three pairs of pelvic bones (two iliac, gluteal and pubic). In a newborn baby, the bones of the pelvic girdle are connected by cartilage.
From 5-6 years old, the fusion of the vertebrae of the sacral spine and the pelvic bones begins, which ends at 17-18 years old. Until this age, it is very dangerous for children to jump from a great height (more than 0.7-0.8 m), especially for girls, as this can lead to displacement of the pelvic bones and their abnormal growth. As a result, various disorders of the development of the pelvic organs can occur, and in girls, as future women, complications during pregnancy and childbirth can occur. Lifting and carrying heavy things (up to 13-15 years old - more than 10 kg), or the constant use of high-heeled shoes by girls under 13-14 years old (dangerous shoe heel height for children is not more than 3 cm) can also lead to similar consequences.
The skeleton of the free lower limb consists of the femur, small and big bones shins and bones of the foot. The foot is formed by the bones of the tarsus (7 bones), metatarsus (5 bones) and phalanges of the fingers (such as on the hand). All bones of the foot are connected by strong bonds and when normal development the foot itself acquires concave crypt, which provides the effect of a spring (shock absorber) and is associated with a person's upright posture. The crypt-shaped foot significantly reduces body tremors when walking, running and carrying weights. A newborn child does not have a crypt (arch) of the foot and it is flat. The crypt of the foot is formed when the child begins to walk and is finally fixed at the age of 14-16. When standing for a long time, sitting, carrying significant loads, when using a narrow foot and overheating the foot, when jumping from a height more than them, the ligaments of the foot in children can stretch and then the foot is reduced to flattening. A person with flat feet gets tired quickly when walking and standing, reduces the speed of running, jumping and, in fact, is a certain disabled person. To prevent flattening of the foot, walking barefoot (especially on sand or pebbles), physical exercises to strengthen the ligaments of the foot, moderate jumping, jogging, motor sports games, using comfortable shoes... You can assess the condition of the foot by taking an imprint of the foot on the floor or on paper (for example, a wet foot on a piece of newspaper). In fig. 26 shows the shape of the foot with varying degrees flattening. The presence of flattening of the foot can be objectively assessed using the plantographic technique of V.A.Yaralov-Yaralenda. For this on

two lines are applied to the foot print (Figure 27): AB, connecting the middle of the heel with the middle of the base thumb and AC, which connects the middle of the heel to the second between the toes.
If the inner fold of the footprint contour does not reach the AC line, or only reaches it, then a normal foot is ascertained (I) if the print contour is between AB and AC lines, then the foot is flattened (II), and if the footprint contour reaches only the line AB then the foot is flat (III). The skeleton of the upper and lower extremities in children develops up to 18-20 years. From 6-7 years old, boys and girls begin intensive processes of ossification of the small bones of the wrist, but at 10-12 years old, gender differences begin to appear in the speed of ossification processes: in boys, these processes slow down and ossification is delayed by 1-1.5 years. Ossification of the phalanges of the fingers in most children ends at the age of 11-12, and the wrists at the age of 12-13 are associated, for example, with the consolidation of the final handwriting of the letter. The bone of the hand of children is not formed quickly (for example, with prolonged physical activity, or a letter). At the same time, moderate and affordable physical movement contribute to the development and even for the time being, delay the processes of ossification. For example, playing musical instruments delays the ossification of the bones of the flanks of the fingers and they grow longer in length - the so-called "pianist's fingers" grow.
The skeleton of the head in humans is called the skull and combines two sections: cerebral and facial. The skull consists of about 23 bones, which in a child are connected by cartilage, except for the lower jaw, which has a joint. The main bones of the cerebral section of the skull are the odd frontal, sphenoid, ethmoid and occipital bones, as well as the paired parietal and temporal bones. In the facial part of the skull, the paired bones are the lacrimal, nasal, zygomatic (cheekbones), upper jaw and palate, and not paired - the lower jaw and the hyoid bone. The skull bones grow most rapidly in the first year of life; from the same period, the cartilaginous joints of the bones gradually begin to be replaced by bone tissue - bone growth occurs through the formation of sutures. With age, the proportions of the parts of the skull change significantly in a child: in a newborn child, the brain section is 6 times larger than the facial one, while in an adult it is only 2-2.5 times. The growth of the skull bones occurs at the age of 20-25.
The proportionality of the development of individual parts of the skeleton is assessed by the ratio of the height of the head to the height of a person. For a newborn, it is approximately 1: 4; at 2 years old - 1: 5; at 6-9 years old - 1: 6; in adults - 1: 7.
The human muscular system consists of three types of muscles: skeletal muscles, heart muscles and smooth muscles of internal organs and blood vessels. The active part of the musculoskeletal system is skeletal muscles, the total number of which in the body is about 600.
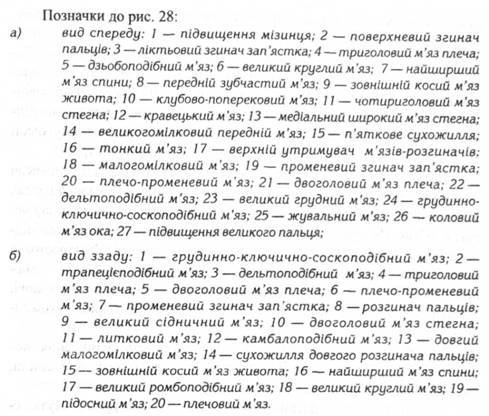
The general layout of skeletal muscles in the human body is shown in Fig. 28. Muscles are broad in shape (for example, the superficial muscles of the trunk, abdomen), short (between the vertebrae of the spine), long (muscles of the limbs, back) circular (muscles around the mouth, eyes, around the holes - the sphincter, etc.). By function, muscles are distinguished - flexors, extensors; leading or diverting; turning inward or outward.

The structural unit of muscles is myofibrils, which is a cocleus (union) of several tens of cells covered with a common membrane. The active elements that ensure the contractile function of muscles are myofilaments (protofibrils) in the form of actin proteins (long and thin filaments) and myosin (short and twice as thick as actin, filaments). In smooth muscles, myofilaments are located irregularly and predominantly along the periphery. inner surface myofibrils. In skeletal muscles, actin and myosin are strictly ordered by a special frame and occupy the entire internal cavity of the myofibril. The places where the actin filaments partially enter Between the filaments of myosin in the microscope look like dark stripes, and other particles - light, therefore such myofibrils are called striated. When the muscle contracts, actin fibers, using the energy of adenosine triphosphoric acid (ATP), move along the myosin fibers, which determines the mechanism of muscle contraction. In this case, myosin acts as an enzyme of adenosine triphosphatase, which promotes the breakdown of ATP and the removal of energy quanta. Due to its structure, smooth muscles contract relatively slowly (from a few seconds to 2-5 minutes). The separated muscles are able to contract very quickly (in a split second).
Formed skeletal muscle consists of bundles of tens of thousands of myofibrils, covered by a common membrane called fascia. The places where muscle fibers are located directly are called abdominal muscles. Tendon processes usually grow along the edges of the abdomen to attach to bones or other muscles. The process from which the muscle begins is called the head, and the opposite is called the tail of the muscle. Based on this, the muscles are 1, 2, 3 and 4 heads. Tails where any muscles can grow together, forming wide tendon links - aponeuroses.
All muscles in the human body, depending on their placement, are divided into mimic and chewing muscles of the face, muscles of the head, neck, back, chest, abdomen and muscles of the upper and lower extremities.
In the process of a child's development, individual muscles and muscle groups grow unevenly: first (at the age of up to one year), the chewing muscles of the face, muscles of the abdomen and back develop rapidly; at the age of 1-5 years, the muscles of the chest, back and limbs develop most intensively. V teenage years the connections of bones and tendons grow rapidly, and the muscles become long and thin, since they do not have time to grow in the wake of the increase in body length. After 15-17 years of age, the muscles gradually acquire the shapes and sizes that are characteristic of adults. With physical training, muscle development can last up to 25-32 years, and the muscles themselves can become impressive in size.
The most important quality of muscles is their strength, which depends on the number of muscle fibers (myofibrils) per unit area of the muscle bar. It has been established that 1 cm2 of the muscle bar is capable of developing forces up to 30 kg. Muscles can do static or dynamic work. Under static load, certain muscles for a long time are in a contracted (tense) state, for example, when exercising on rings, or when lifting and maintaining a barbell. Static loading requires the simultaneous contraction of many muscles in the body and therefore causes rapid fatigue. During dynamic work, individual muscles contract in turn; the acts of contraction quickly change to relaxation, and therefore fatigue sets in much more slowly.
Muscle stress is necessary condition their development and existence. Without work, muscles experience atrophy (decrease, death) and lose their ability to work. The opposite effect is provided by physical training, through which strength, endurance and performance can be significantly increased.
All muscles of a person, even during rest and sleep, are partially tense, that is, they are in a certain tone, which is necessary to maintain the work of internal organs, to maintain the shape and spatial posture of the body. Muscle tone is provided by continuous nerve impulses from motor neurons of the brainstem (located in the red nuclei of the midbrain). Maintaining consistent skeletal muscle tone has great importance to coordinate movements and ensure constant readiness of muscles for activity.
In a child of the first year of life, muscles make up only 16% of body weight, at 3-5 years old - 23.3%, at 7-8 years old - 27% of body weight at 14-15 years old - 33%; at 17-18 years old - 44% of the total body weight. The increase in muscle mass occurs both due to an increase in their length and due to the thickness of the fibers and an increase in the number of muscle myofibrils. In children under 3-4 years of age, the diameter of most skeletal muscles increases relative to a newborn by an average of 2-2.5 times; at 7 years old - 15-20 times, at 20 years - 50-70 times. In general, human muscles can grow up to 30-35 years old.
Muscle strength in children under 3 years old is small, and only from 4-5 years old it begins to gradually grow. At the age of 7-11, the indicators of the muscle strength of children still remain relatively low and therefore power, and especially static, loads lead to rapid fatigue. At this age, children are more able to perform short-term dynamic exercises for speed and strength.
but junior schoolchildren should gradually be taught to maintain static postures, which is especially important for the formation and maintenance of correct body posture.
The most intense muscle strength in both boys and girls grows in adolescence, and starting from 13-14 years old, clear sexual characteristics of the development of muscle strength are manifested: in guys it becomes much more than in girls. The latter should be taken into account when organizing physical education with adolescent girls, limiting the intensity and severity of their loads.
The increase in strength in most muscles lasts up to 25-26 years, and in the flexors - extensors of the limbs - up to 29-30 years.
The uneven development of the strength of various muscle groups must be taken into account when organizing physical education and attracting children to socially useful work.
An important functional indicator of the state of the neuromuscular system is the speed of movements (one-act, or a number of repetitive ones). The speed of one-act movements is especially intensive in younger schoolchildren and at the age of 13-14 approaches the level of adults. From the age of 16-17, the growth rate of this indicator slows down, but the speed of movements continues to gradually increase, reaching a maximum at 25-30 years. It should be noted that the increase in the speed of motor acts with the age of the child is associated with an increase in the speed of conduction of nerve impulses along the nerves, as well as with an increase in the speed of transmission of excitations in the neuromuscular synapses. This effect is due, respectively, to the processes of myelination of nerve fibers (axons) and an increase in the number of synapses and the maturation of the latter.
With age, children also increase the speed of movements, which are repeated. This quality develops most intensively in younger schoolchildren. In the period from 7 to 9 years, the average annual increase in the speed of movements is 0.3-0.6 movements per second (s). In the period of 10-11 years, the rate of increase in speed complex movements slow down (0.1-0.2 movements per s) and grow again (an increase of up to 0.3-0.4 movements per s) at 12-13 years old. The maximum frequency of movements (up to 6-8 movements per second) in boys is established at 15 years old, and in girls - at 14 years old, and then this indicator hardly changes with age. It is believed that an increase in the frequency of movements is associated with an increase in the mobility of nervous processes and with the development of a mechanism for a faster switching of muscles - antagonists (flexors - extensors) from a state of excitement to a state of inhibition and vice versa. The development of the speed of both one-act and complex motor acts in children can be significantly special training, if this is done precisely during the period of primary school age.
An important quality of motor acts is their accuracy, which also changes significantly with age: children up to 5 years old find it difficult to make precise movements; in the primary school period, the accuracy of movements increases significantly and from about 9-10 years old children are able to perform movements with accuracy at the level of adults. Mastering the accuracy of movements is associated with the maturation of the higher centers for the regulation of motor actions and with the improvement of reflex pathways, namely, with the processes of myelination of nerve fibers. Along with the development of the accuracy of movements, children develop the ability to coordinate the level muscle tension... In children of primary school age, this quality is not yet sufficiently developed, and is finally formed only at the age of 11-16. The development of accuracy of movements and the ability to static muscle tension significantly contribute to mastering calligraphic writing, performing complex labor operations (working with plasticine, sawing, etc.), and special physical exercises in the classroom physical culture such as gymnastics, table tennis, ball games and exercises.
An important quality physical development children is the formation of their endurance, including the endurance of skeletal muscles "
Endurance to dynamic work in children of primary school age (7-11 years old) is still very low and only from 11-12 years old it begins to gradually grow, reaching about 50-70% at 14 years old, and 80% of that endurance at 16 years old having adults.
The endurance to static efforts in children gradually increases from 8 to 17 years old, and this happens most intensively in younger schoolchildren. At the age of 17-18, static endurance reaches 85% of that in adults. Finally, the endurance to dynamic and static forces reaches a maximum at 25-30 years. Development of all kinds
endurance is promoted by long walking, running, swimming, sport games(football, volleyball, basketball, etc.).
Thus, the development of many motor qualities in children occurs in the period of primary school age, which gives grounds to recommend for this category of children as widely as possible to introduce measures of purposeful influence on the development of their motor activity, including by organizing special classes in physical education lessons and during sports training.
THEME №3
Skeleton growth and development.
The system of organs of movement includes bones, ligaments, joints and muscles.
Bones, ligaments and joints are passive elements organs of movement.
Muscles are the active part of the movement apparatus..
The system of organs of movement is a single whole: each part and organ is formed in constant communication and interaction with each other.
The skeleton is the support of soft tissues, and where the connected bones form cavities, it performs protective function(skull, chest, pelvis). The skeleton consists of individual bones, interconnected by connective tissue, and sometimes directly bone to bone.
Joint. There are two main types of skeletal joints: discontinuous and continuous.
Continuous connection characterized by the fact that the bones are connected to each other by a continuous layer of tissue and there is no space between them. Movement in this case is limited or excluded. Continuous joints of bones include the skull, pelvis, spine, the junction of the ribs with the sternum.
Discontinuous connection, or joints, characterized by the presence of a small space between the ends of the bones. The ends themselves are enclosed in a special hermetic formation called a bag of the joint. In this case, the ends of the bones are covered with a layer of smooth articular cartilage, and the bag is lined from the inside with a special membrane called synovial. In the joint capsule, constant pressure is maintained, it is below atmospheric. There is a small amount of fluid inside the joint capsule, which reduces the friction of the surfaces against each other.
The articular surfaces of the bones usually correspond in shape to each other, and if one has a head, then the other has a depression for it.
Outside, and sometimes also inside the joints, there are ligaments that strengthen the articulation of the surfaces. Such intra-articular ligaments are found in the hip, knee and other joints.
Scull. In the skeleton of the head - the skull is distinguished facial and cerebral departments.
In the cerebral section of the skull, the brain and the higher sense organs (vision, hearing, smell, etc.) are located, and in the facial - the upper Airways and the initial section of the digestive system.
All bones of the skull, except for the lower jaw and the hyoid bone, have a continuous suture connection. The joints are clearly visible on the skull. Distinguish toothed, scaly and flat seams
A serrated suture is a connection when the projections of the edge of one bone come between the projections of the other, for example, the suture between the frontal and parietal bones. When the edge of one bone overlaps the edge of another, the joint is called a squamous suture, such as the joint between the temporal bone and the parietal. Sometimes the smooth edges of the fused bones are interconnected without any protrusions. It is a flat junction of bones, such as the junction of the nasal bones, upper jaws, etc. temporal bones has an intermittent connection by means of two movable combined mandibular joints... They are formed by the heads of the articular processes of the lower jaw and the depressions of the temporal bones.
In a younger schoolchild, the skull differs from that of an adult in a relatively large size. This symptom is especially noticeable in young children and preschoolers. In addition, it is characterized by the predominance of the brain department over
The development of the cerebral part of the skull depends on the growth and development of the brain, and the development of the facial part depends on teething, the development of the jaws, and especially on the act of chewing.
There are four periods in the development of the skull. The first period - from birth to seven years old... The skull grows evenly. The fontanelles are overgrown. The cranial sutures grow together by the age of 4. By the end of the period, the base of the skull and the foramen magnum reach an almost constant size.
The second period is from 13 to 15 years old. This time intensive growth frontal bones, the predominance of the development of the facial skull over the brain. Add up common features persons who subsequently hardly change.
The third period is from the onset of puberty to 30 years, when the seams of the skull roof become almost invisible.
In younger schoolchildren and adolescents, there is a significant thinness of the skull bones with unclear muscle attachment sites. They also have insufficiently developed mastoid process of the temporal bone.
Torso skeleton.Spine, or vertebral column consists of separate segments - vertebrae, superimposed on each other, and layers of cartilage - intervertebral discs, which give the spine flexibility and resist the load along its longitudinal axis. There are 33-34 vertebrae.
The spine is the axis and support of the skeleton, protects the inside of it spinal cord, takes on the weight of the upper and lower extremities.
As the spine develops, the cartilage tissue decreases. The spine ossifies gradually.
In the spine of an adult, 4 physiological bends are clearly visible: cervical lordosis, thoracic kyphosis, lumbar lordosis and sacrococcygeal kyphosis.
The curves of the spine provide correct position center of gravity and the ability to stand upright.
Lifting weights that are unbearable for a younger student increases lumbar lordosis. Thoracic kyphosis of a schoolchild is more sharply formed when sitting at a desk, especially in children with weakened muscles of the back and neck. The mobility of the spine and its springy property depend on the thickness of the intervertebral cartilage, their elasticity, as well as on the condition of the spinal ligaments. These devices in children are the most elastic, and therefore their spine is very mobile.
Rib cage consists of sternum and ribs, connected to the back of the spine
The sternum consists of three parts (handle, body and xiphoid process). In children, these parts are connected by cartilaginous layers. The body of the sternum consists of segments of cancellous bone. It retains cartilaginous layers for a long time in children. So, the lower segments grow together with the body only by 15-16 years, and the upper ones - by 21-25, much later the xiphoid process grows to the sternum (after 30 years).
The handle of the sternum grows to the body even later than the xiphoid process, and sometimes does not grow at all. The greatest annual growth of the sternum as a whole falls on the 8th year of life in both boys and girls.
Twelve pairs ribs, having the form of narrow, strongly curved plates, articulated with the posterior ends with the spine, their anterior ends (except for the two lower ribs) are articulated with the sternum.
Limb skeleton.
Upper limbs represented by bones shoulder girdle and free upper limb
Shoulder girdle on each side consists of two bones: shoulder blades and collarbone., They are interconnected by ligaments and cartilaginous adhesions, and with the trunk - \ muscles and tendons.
The connection of the bones of the shoulder girdle with bones free limb is carried out thanks to the joints, articular bags and ligaments that strengthen the connection.
Movable connection of the bones of the shoulder girdle with chest and the spine, as well as with a free upper limb, increases the range of motion of the limb.
The shoulder blades of younger schoolchildren are not only smaller in size, but have a smaller concavity of the vertebral surface, which does not correspond to the curvature of the ribs, and therefore some protrusion of the shoulder blades is noted in children. This can be observed with insufficient development of the subcutaneous fat layer and poor development of the muscular system.
The clavicles have a rounder body, they are smaller, more delicate in structure and contain a significant amount of cartilage at the scapular ends. Ossification of the clavicles ends by 20-25 years.
Ossification of the radius ends by 21-25 and ulna by 21-24 years. Ossification of the sesamoid bones (that is, lying in the tendon formations) in boys begins at 13-14 years old, and in girls at 12-13, that is, during puberty. Ossification of the ends (epiphyses) of the tubular bones of the upper extremities ends at 9-11 years, the main phalanges of the fingers and heads of the carpal bones - at 16-17 years, and ossification of the hand - by 6-7 years. Ossification is used to determine "bone age".
Lower limb each side consists of pelvic bone and bones of the free lower limb.
The pelvic bone on the right and left sides is connected to the sacrum bone in adults, and in younger schoolchildren with the sacral vertebrae, forming a pelvis.
A child's pelvic bone is made up of three separate bones: iliac, sciatic and pubic, interconnected by cartilage tissue. Their fusion begins at the age of 5-6 and ends by the age of 17-18. At the place of fusion of the three bones, a thickening is formed with the presence in it of a significant depression for the head of the femur, called acetabulum.
The pelvis as a whole plays a protective role for the pelvic organs and a supporting role for the entire overlying part of the body.
The female and male pelvis have distinctive sexual characteristics. The female pelvis is much wider and lower than the male, its bones are thinner and smoother. The wings of the ilium in women are more turned away, the cape protrudes less, and the pubic angle is more obtuse than in men. The sciatic tubercles in women are more widely spaced from each other. All signs female pelvis associated with fertility. They become especially noticeable from 11 to 12 years old, although the pubic angle is already clearly visible from the age of 5.
Deformation of the pelvic bones in children, especially in adolescent girls, occurs from wearing shoes pa high heels... This leads to a narrowing of the outlet from the pelvis, which makes labor difficult.
TO pelvic bones joins the articulation of the bones of the free lower limb, consisting of the femur, tibia and fibula and the bones of the foot. These are mainly long tubular bones.
Ossification of the lower limb begins in the prenatal period, and ends at different times.
From the age of 7, boys' legs grow faster than girls. And in relation to the body, they reach the greatest length in girls by the age of 13, and in boys by 15.
The bodies of the tubular bones of the lower extremities and their end sections in primary school age are built of bone tissue. And only at the junction (fusion) there are cartilaginous zones that begin to decrease from 12-14 years old and completely disappear at 18-24 years old, turning into bone tissue.
All bones of the foot form an arch, which is noticeable when there is a ligamentous apparatus on the foot. The foot performs a supporting and spring function, the outer edge is the supporting one, and the spring one is the inner one, in which there is a vault.