How prenatal screening is done. What types of tests are performed to screen for the risk of fetal malformations? To do or not to do prenatal screening
During pregnancy, most expectant mothers take great amount analyzes, undergo various manipulations and diagnostic procedures. An important component of these examinations is prenatal screening tests: ultrasound diagnostics in combination with biochemical screening. They are carried out with the aim of detecting the risks of dangerous chromosomal abnormalities in the fetus.
This set of studies can be carried out twice. The first time is at 10-13 weeks of intrauterine development of the fetus, and this is called prenatal screening of the 1st trimester of pregnancy. The second time is to check the results, the tests are taken at 16-18 weeks, this is a screening of the 2nd trimester. The first screening is also called a double test and the second is called a triple test. This is due to the number of tests that a woman must pass. There is also screening for 3 periods of pregnancy.
With the help of biochemical screening in combination with ultrasound, it is possible to determine the risks of such pathologies as trisomies, defects in the development of various organ systems, etc., in an unborn child. For the study, the venous blood of the mother is taken, which is further into laboratory conditions are examined for markers (hormones) associated with pregnancy. This takes 1.5 to 2 weeks.
If a specialist doctor suspects high risks of having a sick child, the woman is sent for consultation and additional examinations for genetics.
Biochemical prenatal screening has a number of positive and negative aspects. The advantages of this method are its non-invasiveness, in contrast to amniocentesis, cordocentesis, the absence of the likelihood of spontaneous abortion during the procedure, sufficiently informative indicators of the risk of having a sick child. However, it is worth remembering about negative sides of this method.
The main disadvantages include the possibility of a false positive and false negative result. In the first case, if absolutely healthy child the test shows a high risk of pathologies, in the second - on the contrary. But be that as it may, the gynecologist who leads a woman's pregnancy is obliged to send the expectant mother for an additional examination before making any decisions.
What tests are included in the list of prenatal biochemical screening?

The complex of analyzes of biochemical prenatal screening of the 1st trimester of pregnancy includes the determination of the level:
- Free β-subunit of human chorionic gonadotropin;
- Pregnancy associated protein A (PAPP-A).
In addition, the examination will be inaccurate if an ultrasound is not performed. This diagnostic method must be passed before laboratory research to find out the exact age of the fetus, determine the coccygeal-parietal size, as well as the thickness of the collar space.
If, for any reason, it is necessary to retest, then this happens at 16-18 weeks of pregnancy, in the 2nd trimester. During this period, they study:
- β-subunit of human chorionic gonadotropin (hCG);
- Alpha-fetoprotein (AFP);
- Free estriol (unconjugated estriol).
These markers are determined after the woman will pass ultrasound diagnostics.
Decoding of the data of prenatal screening of the 1st trimester
With an ultrasound examination, the coccygeal-parietal size should be equal to 45.85 mm or more. The thickness of the collar space is less than 3 mm. The age of the fetus for the informativeness of the test is from 10 to 13 weeks.

HCG at 10-13 weeks of gestation is normally 20 thousand - 90 thousand IU / ml. If the indicators are above the norm, then one can suspect:
- Down syndrome in the fetus;
- Pronounced fetal anomalies;
- Multiple pregnancy;
- Diabetes mellitus in a pregnant woman.
- Taking some groups of drugs.
If the hCG values are below 20 thousand IU / ml, this may indicate:
- About a frozen pregnancy;
- On the lag in the development of the fetus;
- The high risk of spontaneous abortion;
- The presence of severe chromosomal defects in the fetus.
When testing blood for pregnancy associated protein A (PAPP-A), the expected rate ranges from 0.46 to 8.54 mU / ml. Each week of pregnancy has its own regulatory framework for this marker. If its level is less than the lower limit of the norm, we can assume:
- Non-developing pregnancy;
- The threat of spontaneous abortion;
- Abnormalities in the fetus at the chromosomal level (Down syndrome, Cornelia de Lange, Edwards and others).
The increased rates of this study have no diagnostic value. They can only indicate a multiple pregnancy.
Decoding of prenatal screening data for the 2nd trimester
As with the first study, you first need to undergo an ultrasound scan. This time, doctors are interested in biparietal size. After it is installed and all indicators of the fetus are studied using ultrasound, the woman undergoes a triple test.
When decoding analyzes for alpha-fetoprotein (AFP) from 16 to 18 weeks of pregnancy, the following norms are established: 15–95 U / ml. If the indicators are below normal, then risks are likely:
- Abnormalities in the fetus at the chromosomal level (Down syndrome, Edwards);
- Death of the fetus.
At elevated level AFP there are risks:
- Developmental pathologies internal organs;
- Developmental pathologies nervous system.
The second laboratory analysis in the triple test is the determination of unconjugated estriol, the norms of which range from 6.6 to 25 nmol / l. In the case of a reduced level, there are risks:
- Placental insufficiency;
- Delayed delivery;
- Chromosomal abnormalities;
- Infectious processes in the fetus.
An increased level of this marker is not used to diagnose pathologies. It can only show the likelihood of multiple pregnancies, large sizes fetus and the presence of certain diseases in the expectant mother.
As in the first screening, in the second, the rate of hCG is also determined, since this hormone accompanies the entire period of pregnancy. It gradually increases, and then stabilizes and maintains its concentration until the end of pregnancy. At 16-18 weeks of gestation, the norm is 8000-57000 mU / ml.
Some time ago, pregnant women did not know about such a procedure as prenatal or perinatal ... Now all expectant mothers are undergoing such an examination.
What is pregnancy screening, why is it done and why are its results so important? Answers to these and other questions of concern to many pregnant women about perinatal screening we have tried to give in this material.
In order to exclude in the future any misunderstanding of the information presented, before proceeding directly to the consideration of the above indicated topics, it is worth defining some medical terms.
Prenatal screening Is a special kind of a really standard procedure like screening. This comprehensive examination consists of Ultrasound diagnostics and laboratory research, in this particular case biochemistry of maternal serum. Early detection of some genetic abnormalities - this is the main task of such an analysis during pregnancy as screening.
Prenatal or perinatal means prenatal, and by the term screening in medicine, a number of studies of a large stratum of the population are meant, which are carried out in order to form a so-called "risk group" susceptible to certain diseases.
Can be universal or selective screening .
It means that screening tests make not only pregnant women, but also other categories of people, for example, children of the same age to establish the characteristic this period life diseases.
With help genetic screening doctors can find out not only about the problems in the development of the baby, but also react in time to complications during the course of which a woman may not even suspect.
Often, expectant mothers, having heard that they have to go through this procedure, start to panic and worry in advance. However, there is nothing to be afraid of, you just need to ask the gynecologist in advance why you need screening for pregnant women, when and, most importantly, how this procedure is done.
So, let's start with what is standard screening carried out three times during the entire pregnancy, i.e. in every trimester ... Recall that trimester Is a period of three months.
What it is 1 trimester screening ? First, let's answer a common question about how many weeks it is first trimester of pregnancy ... In gynecology, there are only two ways to reliably establish the period during pregnancy - calendar and obstetric.
The first is based on the day of conception, and the second depends on menstrual cycle preceding fertilization ... That's why I trimester - this is the period that, according to the calendar method, begins the first week from conception and ends with the fourteenth week.
According to the second method, I trimester
Is 12 obstetric weeks. Moreover, in this case, the period is counted from the beginning of the last menstruation. Recently screening
not prescribed to pregnant women. 
However, now many expectant mothers are themselves interested in undergoing such a survey.
In addition, the Ministry of Health strongly recommends that research be ordered for all expectant mothers, without exception.
True, this is done voluntarily, since no one can force a woman to undergo any kind of analysis.
It is worth noting that there are categories of women who are simply obliged, for one reason or another, to pass screening, for example:
- pregnant women from thirty-five years old and on;
- expectant mothers with a history of information about the presence of a threat spontaneous ;
- women who in the first trimester suffered infectious diseases ;
- pregnant women forced for health reasons to take in the early stages prohibited for their position medicines;
- women who have had various genetic abnormalities or abnormalities in fetal development ;
- women who have already given birth to children with any deviations or developmental disabilities ;
- women who have been diagnosed frozen or regressive pregnancy (cessation of fetal development);
- suffering from narcotic or women;
- pregnant women in whose family or in the family of the father of the unborn child cases were recorded hereditary genetic abnormalities .
How long do they do prenatal screening for the 1st trimester ? For the first screening during pregnancy, the period is set in the interval from 11 weeks to 13 obstetric weeks of pregnancy and 6 days. Earlier above the designated time, it makes no sense to conduct this survey because its results will be uninformative and completely useless.
The first ultrasound scan at the 12th week of pregnancy is not done by chance for a woman. Since it is at this time that embryonic and begins fetal or fetal the period of development of the future person.
This means that the embryo turns into a fetus, i.e. occur obvious changes, which speak of the development of a full-fledged living human body. As we said earlier, screening tests Is a complex of measures, which consists of ultrasound diagnostics and blood biochemistry of a woman.
It is important to understand that holding screening ultrasound in 1 trimester during pregnancy plays the same important role, as well as laboratory blood tests. Indeed, in order for geneticists to draw the correct conclusions based on the results of the examination, they need to study both the ultrasound results and the patient's blood biochemistry.
How many weeks the first screening is carried out, we talked, now let's move on to deciphering the results of a comprehensive study. It is really important to consider in more detail the norms established by doctors for the results of the first screening during pregnancy. Of course, only a specialist in this area with the necessary knowledge and, most importantly, experience can give a qualified assessment of the results of the analysis.
We believe that it is advisable for any pregnant woman to know at least general information about the main indicators prenatal screening and their normative values. Indeed, it is common for most expectant mothers to be overly suspicious of everything related to the health of their future child. Therefore, they will be much more comfortable if they know in advance what to expect from the research.
Decoding of screening of the 1st trimester by ultrasound, norms and possible deviations
All women know that during pregnancy they have to undergo an ultrasound examination (hereinafter referred to as ultrasound) more than once, which helps the doctor to track intrauterine development unborn child. To screening ultrasound gave reliable results, you need to prepare in advance for this procedure.
We are sure that the vast majority of pregnant women know how to do this procedure. However, it will not be superfluous to repeat that there are two types of research - transvaginal and transabdominal ... In the first case, the device sensor is inserted directly into the vagina, and in the second it contacts the surface of the anterior abdominal wall.

There are no special preparation rules for the transvaginal type of ultrasound.
If you have a transabdominal examination, then before the procedure (about 4 hours before the ultrasound), you should not go to the toilet "on a small", and in half an hour it is recommended to drink up to 600 ml of plain water.
The thing is that the examination must be carried out necessarily on the filled with liquid bladder .
In order for the doctor to obtain a reliable result Ultrasound screening, the following conditions must be met:
- examination period - from 11 to 13 obstetric week;
- the position of the fetus should allow the specialist to carry out the necessary manipulations, otherwise the mother will have to "influence" the baby to roll over;
- coccygeal-parietal size (hereinafter referred to as CTE) should not be less than 45 mm.
What is CTE during pregnancy on ultrasound
When conducting an ultrasound scan, a specialist in mandatory examines various parameters or sizes of the fetus. This information allows you to determine how well the baby is formed, and whether he is developing correctly. The rates of these indicators depend on the duration of pregnancy.
If the value of one or another parameter obtained as a result of ultrasound deviates from the norm up or down, then this is considered a signal of the presence of some pathologies. Coccyx-parietal size - This is one of the most important initial indicators of the correct intrauterine development of the fetus.
The CTE value is compared with the weight of the fetus and the gestational age. This indicator is determined by measuring the distance from the bone of the crown of the child to his coccyx. By general rule, the higher the CTE index, the longer the gestation period.

When this indicator slightly exceeds or, on the contrary, is slightly less than the norm, then there is no reason for panic. This only speaks about the peculiarities of the development of this particular child.
If the CTE value deviates from the standards in a large direction, then this signals the development of a large fetus, i.e. Presumably, the weight of the child at birth will exceed the average rate of 3-3.5 kg. In cases where the CTE is significantly less than the standard values, this may be a sign that:
- pregnancy does not develop as it should, in such cases, the doctor should carefully check the fetal heartbeat. If he died in the womb, then the woman needs an urgent health care (scraping of the uterine cavity ), to prevent possible threat health ( development of infertility ) and life ( infection, bleeding );
- the body of a pregnant woman produces an insufficient amount, as a rule, which can lead to a spontaneous miscarriage. In such cases, the doctor prescribes an additional examination for the patient and prescribes medications containing hormones ( , Dufston );
- mother is sick infectious diseases , including venereal;
- the fetus has genetic abnormalities. In such situations, doctors prescribe additional studies along with, which is part of the first screening test.
It is also worth emphasizing that there are often cases when a low CTE indicates an incorrectly established gestational age. This refers to a variant of the norm. All a woman needs in such a situation is to undergo a second ultrasound examination after a while (usually after 7-10 days).
Fetal BPD (biparietal size)
What is BPD on ultrasound during pregnancy? When conducting an ultrasound examination of the fetus in the first trimester, doctors are interested in all the possible characteristics of the unborn child. Since their study gives specialists maximum information about how intrauterine development takes place little man and whether everything is in order with his health.
What is it BPD of the fetus ? First, let's decipher the medical abbreviation. BPR - this is biparietal fetal head size , i.e. distance between walls parietal bones of the skull , in a simple way, the size of the head. This indicator is considered one of the main ones for determining the normal development of a child.
It is important to note that BPD shows not only how well and correctly the baby is developing, but also helps doctors prepare for the upcoming delivery. Since if the size of the head of the unborn child deviates from the norm in a large direction, then he simply will not be able to pass through the birth canal of the mother. In such cases, a planned cesarean section is prescribed.

When BPD deviates from the established norms, this may indicate:
- about the presence of such pathologies incompatible with life in the fetus as cerebral hernia or tumor ;
- about a sufficiently large size of the unborn child, if other basic parameters of the fetus are ahead of the established developmental standards by several weeks;
- about abrupt development, which after a while will return to normal, provided that other basic parameters of the fetus fit into the norms;
- about fetal development brain caused by the presence of infectious diseases in the mother.
The deviation of this indicator to the lower side indicates that the baby's brain is developing incorrectly.
Collar thickness (TVP)
Fetal TBP - what it is? Collar space by fetus or size cervical fold - this is a place (more precisely, an oblong formation), located between the neck and the upper skin membrane of the baby's body, in which there is an accumulation of fluid. The study of this value is carried out when screening the first trimester of pregnancy, since it is at this time that it is possible to measure TVP for the first time, and then analyze it.
Starting from the 14th week of pregnancy, this formation gradually decreases in size and by the 16th week it practically disappears from view. For TVP, certain norms have also been established, which are in direct proportion to the duration of pregnancy.
For example, the norm collar space thickness at 12 weeks should not exceed the range from 0.8 to 2.2 mm. Collar space thickness at 13 weeks should be in the range of 0.7 to 2.5 mm.
It is important to note that for this indicator, experts set averaged minimum values, the deviation from which indicates a thinning of the collar space, which is the same as expansion of TVP considered an anomaly.
![]()
If this indicator does not correspond to the TVP norms indicated in the above table at 12 weeks and at other periods of pregnancy, then such a result most likely indicates the presence of the following chromosomal abnormalities:
- trisomy 13 , a disease known as Patau syndrome, characterized by the presence of an additional 13 chromosome in human cells;
- trisomy on chromosome 21, known to everyone as Down syndrome , a human genetic disorder in which karyotype (i.e. a complete set of chromosomes) is represented by chromosome 47 instead of 46;
- monosomy on the X chromosome , a genomic disease named after the scientists who discovered it Shereshevsky-Turner syndrome, it is characterized by such anomalies of physical development as short stature, as well as sexual infantilism (immaturity);
- trisomy on chromosome 18 Is a chromosomal disease. For Edwards syndrome (second name this disease) is characterized by a plurality of malformations incompatible with life.
Trisomy Is an option aneuploidy , i.e. changes karyotype , in which there is an additional third in the human cell chromosome instead of normal diploid set.
Monosomy Is an option aneuploidy (chromosomal abnormality) , in which there are no chromosomes in the chromosome set.
What are the norms for trisomy 13, 18, 21 installed during pregnancy? It so happens that in the process of cell division, a failure occurs. This phenomenon has received the name in science aneuploidy. Trisomy - This is one of the varieties of aneuploidy, in which, instead of a pair of chromosomes, an extra third chromosome is present in the cell.
In other words, the child inherits from his parents an additional 13, 18 or 21 chromosome, which in turn entails genetic abnormalities that impede normal physical and mental development. Down Syndrome statistically, this is the most common disease caused by the presence of chromosome 21.
Children born with Edwards syndromes the same as in the case of Patau syndrome , usually do not live up to a year, unlike those who are unlucky to be born with Down syndrome ... Such people can live to a ripe old age. However, such a life can rather be called existence, especially in the countries of the post-Soviet space, where these people are considered outcasts and they try to avoid and ignore them.
In order to exclude such anomalies, pregnant women, especially those at risk, must undergo a mandatory screening examination. The researchers argue that the development of genetic abnormalities is in direct proportion to the age of the expectant mother. The younger the woman, the less likely it is that her child will have any abnormalities.
To establish trisomy in the first trimester of pregnancy, a study is carried out collar space of the fetus using ultrasound. In the future, pregnant women periodically take a blood test, in which for geneticists the most important indicators are the level alpha-fetoprotein (AFP), inhibin-A, chorionic gonadotropin (hCG) and estriol .
As mentioned earlier, the risk of having a genetic disorder in a child depends primarily on the age of the mother. However, there are cases when trisomy is recorded in young women. Therefore, doctors at screening study all possible signs of anomalies. It is believed that an experienced ultrasound specialist can identify problems already during the first screening examination.
Signs of Down syndrome, as well as Edwards and Patau
Trisomy 13 is characterized by a sharp decrease in the level PAPP-A (PAPP pregnancy-associated protein (protein) A-plasma ). It is also a marker of this genetic disorder. The same parameters play an important role in determining whether the fetus has Edwards syndrome .
When there is no risk of trisomy 18, normal values PAPP-A and b-hCG (free beta subunit of hCG)
recorded in biochemical analysis blood. If these values deviate from the standards established for each specific gestational age, then, most likely, genetic malformations will be found in the child. 
It is important to note that in the case when, during the first screening, a specialist records signs indicating a risk trisomies , the woman is referred for further examination and consultation with geneticists. To make the final diagnosis, the expectant mother will have to go through procedures such as:
- chorionic biopsy , i.e. obtaining a sample of chorionic tissue to diagnose anomalies;
- amniocentesis- this is puncture of the amniotic membrane to get a sample amniotic fluid for the purpose of their further study in the laboratory;
- placentocentesis (placental biopsy) , given invasive diagnostic method experts take a sample placental tissue using a special puncture needle, which is pierced anterior abdominal wall ;
- cordocentesis , a method for diagnosing genetic abnormalities during pregnancy, in which the umbilical cord blood of the fetus is analyzed.
Unfortunately, if a pregnant woman has undergone any of the above studies and bioscreening and ultrasound the diagnosis of the presence of genetic abnormalities in the fetus was confirmed, doctors will offer to terminate the pregnancy. In addition, unlike standard screening studies, the data invasive examination methods can provoke a number severe complications up to spontaneous miscarriage, so doctors resort to them in a fairly rare number of cases.
Nasal bone - This is a slightly elongated, quadrangular, convex in front of the paired bone of the human face. At the first ultrasound screening, the specialist determines the length of the baby's nose bone. It is believed that in the presence of genetic abnormalities, this bone does not develop correctly, i.e. its ossification occurs later.

Therefore, if nasal bone is absent or its size is too small during the first screening, this indicates the possible presence of various anomalies. It is important to emphasize that the length of the nasal bone is measured at 13 weeks or 12 weeks. At 11 weeks of screening, the specialist checks only for its presence.
It is worth emphasizing that if the size of the nasal bone does not correspond to the established norms, but if other basic indicators correspond, there is really no reason for concern. This state of affairs may be due to the individual characteristics of the development of this particular child.
Heart rate (HR)
A parameter such as Heart rate plays an important role not only in the early stages, but throughout pregnancy. Constantly measure and monitor fetal heart rate it is necessary already only in order to notice deviations in time and, if necessary, save the life of the baby.
The interesting thing is that though myocardium (heart muscle) begins to decrease already in the third week after conception, you can hear the heartbeat only from the sixth obstetric week. It is believed that at the initial stage of fetal development, the rhythm of its heartbeats should correspond to the mother's pulse (on average, it is 83 beats per minute).
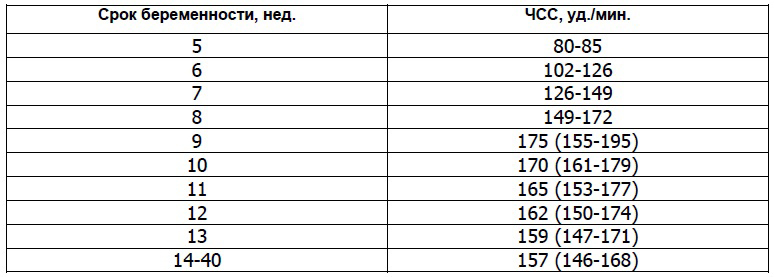
However, already in the first month of intrauterine life, the number of baby's heartbeats will gradually increase (by about 3 beats per minute every day) and by the ninth week of pregnancy it will reach 175 beats per minute. Determine the fetal heart rate using ultrasound.
When conducting the first ultrasound, specialists pay attention not only to the heart rate, but also watch how the baby's heart develops. For this, the so-called four-chamber cut , i.e. methodology instrumental diagnostics malformations of the heart.
It is important to emphasize that a deviation from the standards of such an indicator as heart rate indicates the presence of malformations of the heart ... Therefore, doctors carefully study the structure on a cut atria and fetal heart ventricles ... If any deviations are found, specialists refer the pregnant woman for additional research, for example, to echocardiography (ECG) with dopplerography.
Starting from the twentieth week, the gynecologist of the antenatal clinic will listen to the baby's heart using a special tube at each scheduled visit to the pregnant woman. A procedure such as auscultation of the heart does not apply at an earlier date due to its ineffectiveness, since the doctor simply cannot hear the heartbeat.
However, as the baby develops, his heart will be heard more clearly each time. Auscultation helps the gynecologist determine the position of the fetus in the womb. For example, if the heart is better heard at the level of the mother's navel, then the child is in a transverse position, if the navel is on the left or below, then the fetus is in cephalic presentation , and if above the navel, then in pelvic .
From 32 weeks of gestation, they use cardiotocography (abbreviated CTE ). When carrying out the above types of examinations, a specialist can record in the fetus:
- bradycardia , i.e. abnormally low heart rate , which is usually temporary. This deviation may be a symptom of the mother's autoimmune diseases, anemia, as well as cord clamping when the unborn baby is not getting enough oxygen. Bradycardia can be caused by congenital heart defects in order to exclude or confirm this diagnosis, a woman is sent for additional examinations without fail;
- , i.e. high heart rate. Experts rarely record such a deviation. However, if the heart rate is much higher than that provided for by the norms, then this indicates the mother or hypoxia , development intrauterine infections, anemia and genetic abnormalities at the fetus. In addition, the medications a woman takes can affect heart rate.
In addition to the above characteristics, during the first screening ultrasound examination, specialists also analyze the data:
- about symmetry cerebral hemispheres fetus;
- about the size of the circumference of his head;
- about the distance from the occipital to the frontal bone;
- the length of the bones of the shoulders, thighs and forearms;
- about the structure of the heart;
- about the location and thickness of the chorion (placenta or "child's place");
- the amount of water (amniotic fluid);
- about the condition of the pharynx cervix mothers;
- the number of vessels in the umbilical cord;
- about absence or presence hypertonicity of the uterus .
As a result of an ultrasound scan, in addition to the genetic abnormalities already discussed above ( monosomy or Shereshevsky-Turner syndrome, trisomy on chromosome 13, 18 and 21 , namely Down, Patau and Edwards syndromes ) the following pathologies in development can be identified:
- neural tube , for example, malformation of the spine (meningomyelocele and meningocele) or cranial hernia (encephalocele) ;
- Cornet de Lange syndrome , an anomaly in which multiple malformations are recorded, entailing both physical abnormalities and mental retardation;
- triploidy , a genetic developmental defect in which a failure occurs in the chromosome set, as a rule, the fetus does not survive in the presence of such a pathology;
- omphalocele , embryonic or umbilical hernia, pathology of the anterior abdominal wall, in which some organs (liver, intestines and others) develop in the hernial sac outside abdominal cavity;
- Smith-Opitz syndrome , a genetic abnormality that affects the processes, which subsequently leads to the development of many severe pathologies, for example, or mental retardation.
Biochemical screening of the 1st trimester
Let's talk in more detail about the second stage of a comprehensive screening examination of pregnant women. What it is biochemical screening of the 1st trimester, and what are the standards established for its main indicators? Actually, biochemical screening Is nothing more than biochemical analysis blood of the future mother.
This study is carried out only after an ultrasound scan. This is due to the fact that, thanks to an ultrasound examination, the doctor establishes the exact duration of pregnancy, on which the normative values of the main indicators of blood biochemistry directly depend. So, remember that you need to go to a biochemical screening only with the results of an ultrasound scan.
How to prepare for your first pregnancy screening
We talked about how they do it, and most importantly, when they do a screening ultrasound, now it is worth paying attention to preparing for the delivery of a biochemical analysis. As with any other blood test, you need to prepare for this test well in advance.
If you want to get a reliable result of biochemical screening, then you will have to exactly follow the following recommendations:
- blood for biochemical screening is given strictly on an empty stomach, doctors do not even recommend drinking plain water, let alone any food;
- a few days before the screening, you should change your usual diet and begin to adhere to a sparing diet, in which you should not eat too fatty and spicy foods (so as not to increase the level), as well as seafood, nuts, chocolate, citrus fruits and other allergenic foods, even if you have not previously had an allergic reaction to anything.
Strict adherence to these recommendations will allow you to get a reliable result of biochemical screening. Believe me, it is better to be patient for a while and give up your favorite delicacies, so that later you do not worry about the results of the analysis. After all, any deviation from the established norms, doctors will interpret as a pathology in the development of the baby.
Quite often, in all kinds of forums devoted to pregnancy and childbirth, women talk about how the results of the first screening, expected with such excitement, turned out to be bad, and they had to do all the procedures again. Fortunately, the pregnant women ended up receiving good news about the health of their babies, since the adjusted results indicated that there was no developmental disability. 
The whole point was that the expectant mothers did not prepare properly for the screening, which ultimately led to the receipt of inaccurate data.
Imagine how many nerves were wasted and bitter tears were shed while women were waiting for new test results.
Such colossal stress does not pass without leaving a trace for the health of any person, and even more so for a pregnant woman.
Biochemical screening of the 1st trimester, interpretation of results
When conducting the first biochemical screening test the main role in diagnosing any abnormalities in the development of the fetus, indicators such as free β-subunit of human chorionic gonadotropin (Further HCG ), and PAPP-A (Plasma Protein A Associated with Pregnancy) ... Let's consider each of them in detail.
PAPP-A - what is it?
As mentioned above, PAPP-A - This is an indicator of a biochemical blood test of a pregnant woman, which helps specialists to establish at an early stage the presence of genetic pathologies in the development of the fetus. The full name of this value sounds like pregnancy associated plasma protein A , which literally means - pregnancy-associated plasma protein A .
It is the protein (protein) A produced by the placenta during pregnancy that is responsible for harmonious development unborn child. Therefore, an indicator such as the level of PAPP-A, calculated at 12 or 13 weeks during pregnancy, is considered a characteristic marker for determining genetic abnormalities.
It is mandatory to pass the analysis to check the PAPP-A level should:
- pregnant women over the age of 35;
- women who have previously given birth to children with genetic developmental disabilities;
- mothers-to-be with family members with genetic developmental disabilities;
- women who have had diseases such as , or shortly before pregnancy;
- pregnant women who have had complications or miscarriages before.
Standard values of such an indicator as PAPP-A depend on the duration of pregnancy. For example, the PAPP-A rate at 12 weeks is 0.79 to 4.76 mU / ml, and at 13 weeks - from 1.03 to 6.01 mU / ml. In cases where, as a result of the test, this indicator deviates from the norm, the doctor prescribes additional studies.
If the analysis reveals a low level of PAPP-A, then this may indicate the presence chromosomal abnormalities in the development of the child, for example, Down syndrome also this signals the risk of spontaneous miscarriage and regressive pregnancy ... When this indicator is increased, then this is most likely the result of the fact that the doctor could not calculate the correct gestational age.
That is why blood biochemistry is taken only after an ultrasound scan. However high PAPP-A may indicate the likelihood of developing genetic abnormalities in the development of the fetus. Therefore, in case of any deviation from the norm, the doctor will send the woman for additional examination.
Scientists gave this name to this hormone for a reason, since it is thanks to it that one can reliably find out about pregnancy already 6-8 days after fertilization has occurred egg cells. It is noteworthy that HCG begins to develop chorionic already in the first hours of pregnancy.
Moreover, its level is growing rapidly and already by 11-12 weeks of pregnancy exceeds the initial values by a factor of thousands. Then is gradually losing ground, and its indicators remain unchanged (starting from the second trimester) until childbirth. All pregnancy test strips contain hCG.

If the level human chorionic gonadotropin increased, then this may indicate:
- about the presence of the fetus Down syndrome ;
- O multiple pregnancy ;
- about the development of the mother;
When the hCG level is below the prescribed standards, it says:
- about the possible Edwards syndrome at the fetus;
- about the risk miscarriage ;
- O placental insufficiency .
After a pregnant woman has undergone an ultrasound scan and blood biochemistry, a specialist must decipher the results of the examination, as well as calculate possible risks development of genetic abnormalities or other pathologies using a special computer program PRISCA (Prisca).
The screening summary sheet will contain the following information:
- about age risk developmental anomalies (depending on the age of the pregnant woman, possible deviations change);
- about the values of the biochemical parameters of a woman's blood test;
- about the risk of possible diseases;
- MoM coefficient .
In order to calculate as reliably as possible the possible risks of developing certain abnormalities in the fetus, experts calculate the so-called MoM (multiple of median) coefficient. To do this, all the screening data obtained is entered into a program that plots the deviation of each indicator of the analysis of a particular woman from the average norm established for most pregnant women.
MoM is considered normal if it does not go beyond the range of values from 0.5 to 2.5. In the second stage given coefficient adjusted for age, race, disease (e.g. diabetes ), bad habits(e.g. smoking), the number of previous pregnancies, ECO and other important factors.
On the final stage the specialist makes a final conclusion. Remember, only a doctor can correctly interpret the screening results. In the video below, the doctor explains all the key points related to the first screening.
Screening cost for 1 trimester
The question of how much this study costs and where it is best to take it, worries many women. The thing is that not every state polyclinic can do such a specific examination for free. Based on the reviews left on the forums, many expectant mothers do not trust free medicine at all.
Therefore, you can often come across the question of where to do screening in Moscow or other cities. If we talk about private institutions, then in a fairly well-known and well-proven laboratory INVITRO, biochemical screening can be done for 1600 rubles.
True, this cost does not include ultrasound, which the specialist will definitely ask to present before the biochemical analysis. Therefore, you will have to separately undergo an ultrasound examination in another place, and then go to the laboratory to donate blood. Moreover, this must be done on the same day.
Second screening during pregnancy, when to do and what is included in the study
By recommendations The World Organization Healthcare (hereinafter WHO), every woman is obliged to undergo three screenings throughout the entire period of pregnancy. Although nowadays gynecologists refer all pregnant women for this examination, there are those who, for whatever reason, miss the screening.
However, for some categories of women, such research should be mandatory. This applies primarily to those who have previously given birth to children with genetic or developmental defects. In addition, it is imperative to undergo screening:
- women over the age of 35, since the risk of developing various pathologies in the fetus depends on the age of the mother;
- women who took drugs or other illegal drugs for pregnant women in the first trimester;
- women who have previously suffered two or more miscarriages;
- women who suffer from one of the following inherited diseases to a child - diabetes mellitus, diseases of the musculoskeletal system and of cardio-vascular system, and oncopathology;
- women who are at risk of spontaneous miscarriage.
In addition, future mothers should definitely undergo screening if they or their spouses were exposed to radiation before conception, and also transferred immediately before or during pregnancy. bacterial and infectious diseases ... As with the first screening for the second time, the expectant mother must also do an ultrasound scan and take a biochemical blood test, which is often called a triple test.
Timing of the second screening during pregnancy
So, let's answer the question of how many weeks do the second screening
during pregnancy. As we have already determined, the first study is carried out in the early stages of pregnancy, namely in the period from 11 to 13 weeks of the first trimester. The next screening study is carried out during the so-called "golden" period of pregnancy, i.e. in the second trimester, which starts at 14 weeks and ends at 27 weeks. 
The second trimester is called golden, because it was during this period of time that all the initial ailments associated with pregnancy ( nausea, weakness, and others) retreat, and a woman can fully rejoice in her new state, since she feels a powerful surge of strength.
A woman should visit her gynecologist every two weeks so that she can monitor the progress of her pregnancy.
The doctor gives the expectant mother recommendations regarding her interesting situation, and also informs the woman about what examinations and how long she should undergo. Typically, a pregnant woman takes a urine test and a general blood test before each visit to the gynecologist, and the second screening takes place from 16 to 20 weeks of pregnancy.
Ultrasound screening of the 2nd trimester - what is it?
During the second screening first, they undergo an ultrasound scan to determine the exact duration of pregnancy, so that later specialists can correctly interpret the results of a biochemical blood test. On Ultrasound the doctor examines the development and size of the internal organs of the fetus: bone length, volume chest, head and abdomen, development of the cerebellum, lungs, brain, spine, heart, Bladder, intestines, stomach, eyes, nose, as well as the symmetry of the structure of the face.
In general, everything that is visualized with the help of ultrasound examination... In addition to studying the main characteristics of the baby's development, experts check:
- how the placenta is located;
- the thickness of the placenta and the degree of its maturity;
- the number of vessels in the umbilical cord;
- condition of the walls, appendages and cervix;
- the quantity and quality of amniotic fluid.
Norms for ultrasound screening of the 2nd trimester of pregnancy:
Decoding the triple test (biochemical blood test)
In the second trimester, specialists convert Special attention for such three markers of genetic abnormalities as:
- chorionic gonadotropin - it is produced by the fetal chorion;
- alpha-fetoprotein ( Further AFP ) - this is plasma protein (protein), originally generated corpus luteum, and then produced liver and gastrointestinal tract of the fetus ;
- free estriol ( further hormone E3 ) Is a hormone that is produced in placenta , and fetal liver.
In some cases, they also study the level inhibin (hormone, produced follicles) ... Certain standards are set for each week of pregnancy. It is considered optimal to conduct a triple test at 17 weeks of gestation.
When the level of hCG at the second screening is overestimated, then this may indicate:
- about multiple pregnancy ;
- O diabetes mellitus from the mother;
- about the risk of development Down syndrome if the other two indicators are below normal.
If hCG, on the contrary, is lowered, then this says:
- about the risk Edwards syndrome ;
- O frozen pregnancy;
- O placental insufficiency .
When the AFP level is high, then there is a risk of:
- the presence of developmental abnormalities kidney ;
- defects neural tube ;
- developmental disabilities abdominal wall ;
- damage brain ;
- lack of water ;
- fetal death;
- spontaneous miscarriage;
- emergence rhesus conflict .
Decreased AFP can be a signal:
- Edwards syndrome ;
- diabetes mellitus mothers;
- low location placenta .
At a low level, there is a high risk:
- development anemia at the fetus;
- adrenal and placental insufficiency;
- spontaneous miscarriage ;
- availability Down syndrome ;
- development intrauterine infection ;
- delays in the physical development of the fetus.
It should be noted that the level hormone E3 some medications (for example), as well as improper and unbalanced nutrition of the mother, have an effect. When E3 is elevated, doctors diagnose diseases kidney or multiple pregnancy, and also predict premature birth when the estriol level rises sharply.
After the expectant mother goes through two stages of screening, doctors analyze the information received using a special computer program and calculate the same MoM coefficient as in the first study. The conclusion will indicate the risks for a particular type of deviation.
Values are indicated as a fraction, for example 1: 1500 (i.e. one case per 1500 pregnancies). It is considered the norm if the risk is less than 1: 380. Then the conclusion will indicate that the risk is below the cut-off threshold. If the risk is higher than 1: 380, then the woman will be referred for additional consultation with geneticists or offered to undergo invasive diagnostics.
It should be noted that in cases where at the first screening the biochemical analysis corresponded to the norms (indicators were calculated HCG and PAPP-A ), then the second and third time it is enough for a woman to do only an ultrasound.
Last screening examination future mom takes place in third trimester ... Many people wonder what they are looking at at the third screening and when this study should be done.
As a rule, if the pregnant woman was not diagnosed with any abnormalities in the development of the fetus or during pregnancy at the first or second examination, then she only needs to undergo an ultrasound examination, which will allow the specialist to draw final conclusions about the condition and development of the fetus, as well as its position in the womb. 
Determination of the position of the fetus ( cephalic or breech presentation ) is considered an important preparatory stage before childbirth.
So that the delivery is successful, and the woman can give birth on her own without surgical intervention, the child should be in a cephalic presentation.
Otherwise, doctors are planning a cesarean section.
The third screening includes procedures such as:
- Ultrasound , which all pregnant women go through;
- dopplerography Is a technique that focuses mainly on the state of blood vessels placenta ;
- cardiotocography - a study that allows you to more accurately determine the heart rate of a child in the womb;
- blood biochemistry , during which attention is focused on such markers of genetic and other abnormalities as the level HCG, ɑ-fetoprotein and PAPP-A .
Timing of the third screening during pregnancy
It is worth noting that only the doctor decides at how many 3 weeks a woman should undergo screening, based on individual characteristics this particular pregnancy. However, it is considered optimal when the expectant mother undergoes a planned ultrasound scan at 32 weeks, and then immediately undergoes a biochemical blood test (if indicated), and also undergoes other necessary procedures.
However, for medical reasons, carry out dopplerography or CTG the fetus can be from 28 weeks of gestation. Third trimester starts at 28 weeks and ends with childbirth at 40-43 weeks. The last screening ultrasound is usually prescribed at 32-34 weeks.
Decoding ultrasound
How long does it take for a pregnant woman to undergo the third screening ultrasound, now we will talk in more detail about decoding the study. When conducting an ultrasound scan in the third trimester, the doctor pays special attention to:
- for development and structure of cardio-vascular system a child in order to exclude possible developmental pathologies, for example, heart disease ;
- on correct development brain , organs of the abdominal cavity, spine and genitourinary system;
- on located in the cranial cavity vein of Galen which plays an important role in the proper functioning of the brain in order to exclude aneurysm ;
- on the structure and development of the child's face.
In addition, ultrasound allows the specialist to assess the condition amniotic fluid appendages and uterus mother, as well as check and the thickness of the placenta ... In order to exclude hypoxia and pathology in the development of the nervous and cardiovascular system , as well as to reveal the features of blood flow in vessels of the uterus and the child, as well as in the umbilical cord, spend dopplerography .
As a rule, this procedure is carried out only according to indications simultaneously with an ultrasound scan. In order to exclude fetal hypoxia and define Heart rate, spend CTG ... This type of research focuses exclusively on the baby's heart, so cardiotocography prescribed in cases where the doctor has concerns about the condition cardiovascular child's systems.
Ultrasound in the third trimester of pregnancy allows you to determine not only the presentation of the child, but also the maturity of his lungs, on which the readiness for birth depends. In some cases, hospitalization for early delivery may be required to keep the baby and mother alive.
| Index | Average rate for 32-34 weeks of pregnancy |
| Placenta thickness | from 25 to 43 mm |
| Amniotic (amniotic) index | 80-280 mm |
| Placental maturity | 1-2 degree of ripening |
| Uterine tone | absent |
| Uterine pharynx | closed, length not less than 3 cm |
| Fetal growth | on average 45 cm |
| Fetal weight | on average 2 kg |
| Fetal belly girth | 266 - 285 mm |
| BPR | 85-89 mm |
| Fetal thigh length | 62-66 mm |
| Fetal chest girth | 309-323 mm |
| Fetal forearm size | 46-55 mm |
| Fetal shin bone size | 52-57 mm |
| Fetal Shoulder Length | 55-59 mm |
Based on the results of a biochemical blood test MoM factor should not deviate from the range from 0.5 to 2.5. The risk value for all possible deviations should correspond to 1: 380.
The content of the article:Prenatal screening in our country is carried out on a massive scale, it is carried out for all pregnant women registered in the antenatal clinic. The examination is recommended by the Ministry of Health on the basis of the order of the Russian Federation No. 457 of 2000.
Prenatal screening is a diagnostic method that uses various diagnostic tests and instrumental studies are carried out (ultrasound examination and blood sampling for markers of chromosomal abnormalities are carried out). The examination is carried out at certain stages of pregnancy. Such a complex medical research allows you to identify serious abnormalities in the development of the fetus, chromosomal abnormalities and congenital defects. Thus timely diagnosis helps the gynecologist to determine the tactics of pregnancy management.
Due to the simplicity of prenatal screening, it is possible to check a large number women, if the process is organized logically, then 85-95% of pregnant women are examined. The procedure is available for medical institutions of various levels, since it does not require significant material support. The main devices for prenatal screening are modern ultrasound machines, laboratory instruments and blood diagnostic complexes, which makes it possible to study the level of hormones in the blood donated by pregnant women, both in the early and late stages of pregnancy.
What are the pros and cons of prenatal screening
Benefits of Screening in Pregnant Women
Safe examination method.
Identifies a risk group for chromosomal abnormalities.
Easily accessible and easy to carry.
Free under the compulsory medical insurance policy.
Disadvantages of screening in pregnant women
There may be false positive and false negative results.

What does prenatal screening include?
Ultrasound screening (ultrasound examination).
Biochemical studies to identify certain markers (when they are carried out, they are based on the fact that abnormalities in the development of the fetus are manifested by the presence of certain substances in the mother's body).
Invasive methods (cordocentesis, amnicentesis, chorionic biopsy) are carried out only after ultrasound screening and biochemical blood tests with unfavorable results. Such pregnant women are at risk and one of the invasive techniques will be required to obtain a reliable result. These techniques, in contrast to ultrasound and blood collection, carry the risk of miscarriage and complications of pregnancy, therefore, they are carried out with the written consent of the pregnant woman and after consulting a geneticist.
What pathologies are looked for during prenatal screening
During the screening, it turns out to determine whether the child will be born with one of the following deviations:
- Triplodia(a deviation associated with a change in the number of chromosomes in the cell nucleus).
- Edwards syndrome(the presence of an additional 18th chromosome - three instead of two). Screening is relevant in the same time frame as indicated above.
- Patau syndrome(trisomy 13) - the presence of another copy of the 13th chromosome.
- Shereshevsky-Turner syndrome(absence in the diploid - double - chromosome set of the X chromosome in a female fetus).
- Smith-Lemli-Opitz syndrome(a disease leading to metabolic disorders).
- Corneli de Lange syndrome(an anomaly associated with a mutation in the NIPBL or SMC1A genes).
- Abnormalities in the development of the neural tube(detected at the beginning of the second trimester of pregnancy).
The listed diseases belong to congenital pathologies, as a result, a viable child is born, who has serious deviations in health and developmental disabilities. Cure such genetic disorders modern medicine not able to.
The information obtained during ultrasound screening and blood tests for markers (as mentioned above) are not reliable evidence of fetal malformations, but at the same time give rise to thorough examination pregnant woman using complex techniques and invasive diagnostics. Clarification of the diagnosis and assessment of existing abnormalities allows the doctor to judge whether they pose a threat to the woman's health, whether they can cause an abortion.

During the entire pregnancy, ultrasound screening is carried out three times at certain stages of pregnancy, when the required indicators are most informative. Let's take a closer look at each period of ultrasound screening.
Ultrasound screening: period
An ultrasound examination is carried out at a strictly established period of pregnancy, namely:
First ultrasound diagnostics appointed at -14 weeks of gestation.
Target- during examination, to identify possible serious violations in the formation of the nervous system (anencephaly), signs of chromosomal abnormalities in a child (measuring the thickness of the collar zone, determining the nasal bone), to assess the blood flow in the Arantia (venous) duct.
The second stage of ultrasound screening is performed at -24 weeks of pregnancy.
Target: a study of the condition of the fetus helps to assess the presence or absence of gross anatomical defects of the most important human organs. Such disorders include various abnormalities that cannot be treated after birth, for example, defects in the development of the nervous system, organs of the urinary system, heart and blood vessels, upper and lower extremities.
Ultrasound at 30-32 weeks of gestation is aimed at identifying developmental abnormalities associated with the late onset of pronounced signs of pathology, which, as a rule, are amenable to surgical treatment.

Carrying out only ultrasound examination is not enough, therefore, they resort to the use of laboratory tests. It is important to carry out the diagnosis at a certain time, since the results can be influenced by extraneous factors.
A blood test should be performed immediately after an ultrasound scan at intervals of 1–2 days. Blood should be taken in the morning on an empty stomach, or 3-4 hours after a meal.
Periods of laboratory tests
Double test or first trimester screening... During the first trimester, the procedure is carried out for a period of 10-13 weeks. The analysis evaluates a certain type of hCG ("pregnancy hormone") - free β-subunit; as well as plasma protein A (PAPP-A), which is secreted only during pregnancy.
To get reliable results and draw a conclusion, they pay attention to how the woman's menstrual cycle went. If there is an irregularity in the onset of menstruation, there is a pregnancy that has arisen a short period of time after childbirth, then errors and a decrease in the reliability of the data are possible, since real terms the onset of pregnancy may not coincide with the expected, and the rates of hCG during pregnancy strictly depend on the days after conception.
Triple test or 2nd trimester screening appointed for a period of 14-20 weeks, it is best to carry it out a little later - at 16-18 weeks of pregnancy. During the analysis, three components are assessed:
Total hCG either the β-subunit;
Alpha-fetoprotein or AFP (a protein produced in the liver and gastrointestinal tract of the fetus);
Free estriol (a female sex hormone synthesized in the placenta).
Sometimes it is also possible to test inhibin A, which is present in the blood of pregnant and non-pregnant women.
Screening results in the form of an individual risk assessment
The data obtained as a result of prenatal screening should be formalized in the form of an individual risk assessment. To do this, use special computer programs, they enter data about the patient (exact gestational age, age, weight, race, number of fetuses, history of diabetes mellitus, smoking, pregnancy as a result of IVF, a full list of medications used, the presence of children with genetic pathology in the past), the results of ultrasound and biochemical blood tests.
Programs for obtaining prenatal screening results
There are special programs that imply a comprehensive study, which helps to get results in a shorter time, but at the same time eliminate the likelihood of the influence of the human factor. In Russia, two programs are most often used.
1. PRISCA program
Thanks to the implementation of this method, it is possible to identify whether there is a risk of developing a fetus with Edwards, Down syndromes, to determine the presence of neural tube defects. During the state check, take into account physiological features women, specific traits the course of pregnancy, which is important for IVF fertilization, multiple pregnancies.
2. DELFIA-LifeCycle program
Helps to identify most of the abnormalities that cannot be cured after the baby is born. These include: Patau, Down, Shereshnevsky-Turner, Edwards, Cornelia de Lange syndromes, as well as pathology in the development of the neural tube. Here, too, it turns out to take into account the individual indicators of a woman, the specificity of the course of pregnancy (several fetuses, IVF).
There is no point in just comparing biochemical parameters with norms without regard to risks. Therefore, in the results of prenatal screening, the ratios reflecting the possibility of the fetus to have certain pathologies are taken into account. For example: a risk of 1 in 40 means that out of 40 women who have the same results, only one will have a baby with chromosomal abnormalities, and the other 39 mothers will have healthy children. A risk of 1 in 5000 means that out of 5000 pregnant women with the same result, one will have a child with a genetic disorder, and 4999 mothers will be born healthy babies... That is, what less second the number, the greater the risk of pathology. In addition, the results indicate your performance above or below the cut-off threshold. Most often, the tests use a threshold of 1 to 250. That is, indicators greater than 1: 250 will be considered the norm, and less increase the risk of pathology.

As soon as the results of the screening examination are assessed, the woman will receive information about whether it is possible to give birth to a child with any abnormalities. Further, it is the pregnant woman herself who decides whether to resort to further testing using invasive methods, which will 100% confirm or deny genetic abnormalities. Note! They should only be carried out if the pregnant woman is ready to terminate the pregnancy when adverse results, otherwise they are inappropriate and have risks to complicate the course of pregnancy.
Please note that normal result screening is not a 100% guarantee of the birth of a child without chromosomal abnormalities. They only say that such a probability is very small in percentage terms. On the other side bad results screening does not indicate the presence of pathology in the fetus, but only that it is more likely according to the accumulated statistics. In addition, screening is aimed at identifying common chromosomal abnormalities and neural tube defects, but, unfortunately, there may be other more rare fetal anomalies that screening will not reveal. Hence, many pregnant women are interested in the question of whether it is worth worrying and doing screening or is it better to calmly reach the pregnancy. Let's answer this question.
To do or not to do prenatal screening
As mentioned above, prenatal screening is the recommended procedure for all pregnant women in the Russian Federation. But you have the right to refuse this study. In any case, only you can decide to pass it or not.
Children with genetic defects can be born to absolutely any parents, regardless of the risk group, health status, age and other characteristics, and on the other hand, completely healthy children can be born to parents from the risk group.
Prenatal screening is just a statistic, not a diagnosis. Diagnostics does not pose any danger to the health of the mother and fetus, but at the same time it helps doctors to manage the pregnancy, decide on further examinations, and psychologically prepare the pregnant woman for possible unfavorable options. And for the pregnant woman herself, this is a way to find out about the health of her child.
Invasive methods (chorionic biopsy or placentocentesis, amnicentesis, cordocentesis)
Invasive methods are used if there is a high risk of chromosomal and genetic diseases. The cells and tissues of the fetus or chorion / placenta are taken through the abdominal wall under ultrasound control. Free invasive diagnostics is carried out in the direction of genetics in specialized maternity hospitals.
Chorionic biopsy carried out at a period of 10-14 weeks of pregnancy, cells that form the placenta are taken as a material. The results allow us to judge the chromosome set of the fetus, but due to incomplete coincidence of genomes, a false positive or false negative result is possible, therefore, the reliability of the test is 99%. Chromosomal diseases are determined, and in addition, the test can be used to determine the sex of the child and paternity.
Placentocentesis carried out at a period of 14-16 weeks of pregnancy, placental cells are taken as material. The results are the same as for chorionic biopsy.
Amniocentesis carried out at 16-19 weeks of pregnancy, a small amount of amniotic fluid is taken as a material. The amniotic or amniotic fluid contains vellus hair and epithelial cells of the fetus. Chromosomal and genetic diseases, the degree of Rh-conflict, oxygen starvation or lung maturity are determined.
Cordocentesis carried out after 19 weeks of pregnancy, blood is taken from the umbilical cord of the fetus as a material. It is the most informative method, with the help of it you can determine any deviations as in a biochemical blood test (hormones, biochemistry, immunological indicators, etc.), the presence of infectious or sexually transmitted diseases in the fetus. In addition, cordocentesis can be used as a therapeutic procedure (blood transfusion to the fetus, intravenous drug administration).
When pregnancy occurs, expectant mothers begin to get overwhelmed by fear: is everything all right with the baby? Fortunately, modern diagnostic methods allow early detection of fetal developmental disorders. There is such a thing as prenatal screening. This is nothing more than a complex of instrumental and laboratory research methods designed to identify the risk of developing congenital pathologies.
Table of contents: We recommend reading:There is a certain list of laboratory tests that all pregnant women should undergo. Prenatal screening is not required for everyone, but only for those women who are at a special risk group for congenital anomalies.
So, screening should be done in such cases:
- Pregnant woman over 35;
- If the family already has children with chromosomal abnormalities;
- V obstetric history two or more miscarriages;
- If in the first trimester a woman took medications prohibited during pregnancy;
- The child's parents are close relatives;
- If, before conceiving a child, the parent underwent a course of radiation;
- The threat of termination of pregnancy.
Screening tests are performed every trimester. Research is most important in the first and second trimesters.

Screening of the 1st trimester
The first screening is a screening performed in the first trimester. The most acceptable timing is 10-13 weeks of pregnancy. The first screening allows you to identify congenital malformations at an early stage.
Screening in the first trimester includes:
- Fetal ultrasound;
- Biochemical blood test.
Fetal ultrasound in the first trimester
Allows you to determine the location of organs, the length of the fetal body, head circumference, measure the thickness of the cervical fold, coccygeal-parietal size.
The coccygeal-parietal dimension (CTE) is the length measured from the coccyx to the parietal region of the skull. If, during an ultrasound scan, a specialist has determined that the CTE is less than expected, this may indicate:
- Incorrectly calculated gestational age;
- Violation of fetal development as a result of hormonal, infectious diseases of the mother;
- The presence of genetic pathology;
- Incorrect position of the fetus, which does not allow to fully measure the distance.
Measuring an indicator such as biparietal size (BPD) allows you to study the formation of the brain. Biparietal size is the distance from one temple to the other. A decrease in BPD indicates an underdevelopment of the brain, and an increase indicates dropsy of the brain.
 The likelihood of chromosomal abnormalities can be determined by studying the thickness of the collar space (TVP). An increase in TPV can signal Down syndrome, Edwards, Turner, Patau syndrome.
The likelihood of chromosomal abnormalities can be determined by studying the thickness of the collar space (TVP). An increase in TPV can signal Down syndrome, Edwards, Turner, Patau syndrome.
Equally important in ultrasound examination of the fetus is the determination of the length of the nasal bone. In the presence of chromosomal abnormalities, the formation of the nasal bone is delayed. Accordingly, its absence or small size can signal chromosomal pathology.
Biochemical blood test
For biochemical research, blood is taken from a vein of a pregnant woman. Blood sampling is carried out on an empty stomach in the morning. The greatest interest presents the determination of the levels of human chorionic gonadotropin (hCG), as well as plasma protein (PAPP-A) in the blood of a pregnant woman.
HCG is synthesized by chorionic cells. The level of the hormone correlates with the gestational age. 
Chorionic gonadotropic hormone has two fractions: alpha and beta. For the diagnosis of congenital pathology, the determination of the level of beta-hCG is of the greatest importance. A decrease in hCG below the normal level is observed when ectopic pregnancy, pathology of the placenta, Edwards syndrome. A increasing hCG may indicate:
- Multiple pregnancies;
- Genetic diseases of the fetus.
Determination of the plasma protein PAPP-A is performed from the 8th week of pregnancy. It is noteworthy that the determination of this indicator after the 14th week is no longer so reliable. 
A decrease in PAPP-A in comparison with normal indicators typical for a certain period of pregnancy indicates:
- Chromosomal abnormalities of the fetus;
- Threatened miscarriage.
It is worth noting that an increase in plasma hormone may also indicate the presence of fetal developmental disorders.
Screening in the second trimester, first of all, is carried out to confirm or deny the results of the first screening, as well as if indicated. The second screening is recommended to take place at 16-20 weeks of pregnancy.
Pregnant women undergo such studies:
- Biochemical examination of the fetus (hCG, AFP, estriol).
Ultrasound of the fetus in the second trimester
The need for an ultrasound scan in the second trimester is dictated by the fact that during this period important functional systems, the study of which will assess the development of the child. Ultrasound helps to study:
- Correct formation of the spine, limbs;
- The length of the nasal bone;
- The size of the structures of the brain;
- Functioning of internal organs;
- Basic parameters of the child;
- The size and structure of the placenta;
- Dimensions of the cervix;
- Amniotic fluid level;
- Fetal heart rate;
- The length of the umbilical cord;
- The condition of the appendages of the pregnant woman.
Examination of the placenta allows the doctor to determine its location. Normally, the placenta is located on back wall uterus, approximately 6-8 cm higher from the internal os. If it is located at the bottom of the uterus and closes the internal pharynx, this is a deviation from the norm.
 An equally important role is played by the location of the umbilical cord, normally it attaches to the central region of the placenta. There are other atypical options for the placement of the umbilical cord: marginal, sheath, split. Such abnormalities can lead to difficulties during childbirth, in particular, to fetal freezing.
An equally important role is played by the location of the umbilical cord, normally it attaches to the central region of the placenta. There are other atypical options for the placement of the umbilical cord: marginal, sheath, split. Such abnormalities can lead to difficulties during childbirth, in particular, to fetal freezing.
The umbilical cord has three vessels: two arteries and a vein. If at least one artery is missing, this can lead to a violation of the formation and development of the child's internal organs.
During an ultrasound examination, the doctor can calculate the amniotic fluid level. What can this indicator tell you? With low water there is a risk of the formation of a defect in the limbs, spine, and organs of the nervous system.
Biochemical blood test
Estriol is a hormone responsible for the formation of the placenta. A high level of this hormone can be determined with multiple pregnancies, as well as with a large fetus. A low level can inform about placental insufficiency, the threat of miscarriage, hypoplasia.

Alpha-fetoprotein (AFP) is a protein synthesized by the liver of the fetus. The substance through the placenta enters the mother's body, making it possible to determine its concentration by examining the venous blood of a pregnant woman.
A low ACE level is observed when:
- Down syndrome;
- Edwards Syndrome;
- Bubble drift;
- Fetal death.
A high concentration of alpha-fetoprotein may indicate:
- Hernia in the navel;
- Abnormal formation of the fetal neural tube;
- Abnormal formation of the esophagus or duodenum;
- Meckel syndrome.
 First of all, it should be noted that screening is a complex study. This means that if one of the results is unsatisfactory, and the rest are normal, this does not indicate the presence of pathology. Moreover, even if the results are collectively unsatisfactory, this does not mean that the baby is 100% likely to be born sick. Screening allows you to assess only the degree of likelihood of developing pathology in a particular child.
First of all, it should be noted that screening is a complex study. This means that if one of the results is unsatisfactory, and the rest are normal, this does not indicate the presence of pathology. Moreover, even if the results are collectively unsatisfactory, this does not mean that the baby is 100% likely to be born sick. Screening allows you to assess only the degree of likelihood of developing pathology in a particular child.
If the doctor deems it necessary, he will refer the woman to a geneticist. With a high risk of congenital abnormalities, the pregnant woman is sent for amniocentesis or chorionic villus sampling. Amniocentesis enables a specialist to detect the presence of congenital and hereditary diseases by examining the amniotic fluid.
Chorionic villus sampling can also detect chromosomal abnormalities and genetic diseases.
Remember: the doctor makes a conclusion about the risk of having a baby with pathology based on the results of all screening studies. Having received an unsatisfactory result in your hands, in no case should you panic. The doctor will recommend additional research, the results of which can refute all worries about the child's health.
Grigorova Valeria, medical columnist
The Center for Immunology and Reproduction has been successfully working for many years prenatal screening program... Our specialists are invited to lecture at specialized conferences and in other clinics. Our laboratory receives stable good grades in the quality control system. Specially trained specialists carry out the calculation of risks.
What is prenatal diagnosis?
The word "prenatal" means "prenatal." Therefore, the term "prenatal diagnosis" means any research that allows you to clarify the state of the intrauterine fetus. Since a person's life begins from the moment of conception, various health problems can occur not only after birth, but also before birth. Problems can be different:
- quite harmless, with which the fetus can cope on its own,
- more serious, when timely medical assistance will preserve the health and life of the intrauterine patient,
- quite difficult, which modern medicine cannot cope with.
To find out the state of health of an intrauterine fetus, prenatal diagnostic methods are used, which include ultrasound, cardiotocography, various biochemical studies, etc. All these methods have different capabilities and limitations. Some methods are quite safe, such as ultrasound. Some are associated with certain risks to the fetus, such as amniocentesis (a sample of amniotic fluid) or chorionic villus sampling.
It is clear that prenatal diagnostic methods associated with the risk of pregnancy complications should be used only when there are compelling indications for their use. In order to maximally narrow the circle of patients requiring invasive (i.e., associated with intervention in the body) methods of prenatal diagnosis, selection is used. risk groups the development of certain problems in an intrauterine fetus.
What are risk groups?
Risk groups are such groups of patients, among which the probability of detecting a particular pregnancy pathology is higher than in the entire population (among all women in a given region). There are risk groups for the development of miscarriage, gestosis ( late toxicosis), various complications in childbirth, etc. If a woman, as a result of examination, is at risk for a particular pathology, this does not mean that this pathology will necessarily develop. This only means that in this patient one or another type of pathology may occur with a greater probability than in other women. Thus, the risk group is not the same as the diagnosis. A woman may be at risk, but there may be no problems during pregnancy. And nevertheless, a woman may not be at risk, but she may have a problem. The diagnosis means that this or that pathological condition has already been found in this patient.
Why are risk groups needed?
Knowing that the patient is in a particular risk group helps the doctor to correctly plan the tactics of pregnancy and childbirth. Allocation of risk groups allows you to protect patients who are not at risk from unnecessary medical interventions, and vice versa, allows to justify the appointment of certain procedures or studies to patients at risk.
What is screening?
Screening means screening. In medicine, screening means simple and safe research. large groups population in order to identify risk groups for the development of a particular pathology. Prenatal screening refers to studies performed on pregnant women to identify groups at risk of pregnancy complications. A special case of prenatal screening is screening to identify risk groups for the development of congenital malformations in the fetus. Screening does not allow identifying all women who may have this or that problem, but it makes it possible to single out a relatively small group of patients, within which most of the people with this type of pathology will be concentrated.
Why is fetal malformation screening needed?
Some types of congenital malformations in the fetus are quite common, for example, Down's syndrome (trisomy on the 21st pair of chromosomes or trisomy 21) - in one case per 600 - 800 newborns. This disease, like some other congenital diseases, occurs at the time of conception or at the earliest stages of the embryo's development, and using invasive methods of prenatal diagnosis (chorionic villus sampling and amniocentesis) can be diagnosed at a fairly early stage of pregnancy. However, such methods are associated with the risk of a number of pregnancy complications: miscarriage, the development of a conflict for the Rh factor and blood group, infection of the fetus, the development of hearing loss in a child, etc. In particular, the risk of miscarriage after such studies is 1: 200. Therefore, these studies should only be prescribed to women. high groups risk. Risk groups include women over 35 and especially over 40, as well as patients with the birth of children with developmental defects in the past. However, children with Down syndrome can also be born to very young women. Screening methods - completely safe tests carried out at certain stages of pregnancy - make it possible with a very high degree of probability to identify groups of women at risk of Down syndrome who may be indicated for a chorionic villus sampling or amniocentesis. Women who are not at risk do not need additional invasive studies. Detection high risk the development of fetal malformations using screening methods is not a diagnosis. The diagnosis can be made or rejected with additional tests.
What types of birth defects are screened for?
- Down syndrome (trisomy on the twenty-first pair of chromosomes)
- Edwards syndrome (eighteenth pair trisomy)
- Neural tube defects (spina bifida and anencephaly)
- Smith-Lemli-Opitz syndrome
- Corneli de Lange syndrome
What types of tests are performed to screen for the risk of fetal malformations?
By types of research allocate:
- Biochemical screening: blood test for various indicators
- Ultrasound Screening: identification of signs of developmental anomalies using ultrasound.
- Combined screening: combination of biochemical and ultrasound screenings.
A general trend in the development of prenatal screening is the desire to receive reliable information about the risk of developing certain disorders as early as possible in pregnancy. It turned out that combined screening at the end of the first trimester of pregnancy (10-13 weeks) makes it possible to approach the effectiveness of classical biochemical screening of the second trimester of pregnancy.
Ultrasound screening, used to mathematically evaluate the risks of fetal anomalies, is performed only once: at the end of the first trimester of pregnancy.
Concerning biochemical screening, then the set of indicators will be different at different stages of pregnancy. During pregnancy 10-13 weeks the following indicators are checked:
- free β-subunit of human chorionic hormone (St. β-hCG)
- PAPP-A (pregnancy associated plasma protein A), pregnancy associated plasma protein A
The calculation of the risk of measuring fetal abnormalities, carried out on the basis of the measurement of these indicators, is called double biochemical test of the first trimester of pregnancy.
Using a double test in the first trimester, the risk of detection in the fetus is calculated Down syndrome (T21) and Edwards syndrome (T18), trisomy on chromosome 13 (Patau syndrome), triploidy of maternal origin, Shereshevsky-Turner syndrome without dropsy. The risk of neural tube defects cannot be calculated using a double test, since the key indicator for determining this risk is α-fetoprotein, which begins to be determined only from the second trimester of pregnancy.
Special computer programs make it possible to calculate the combined risk of fetal anomalies, taking into account the biochemical parameters determined in the double test of the first trimester and the results of an ultrasound scan performed at 10-13 weeks of pregnancy. This test is called combined with TVP double test of the first trimester of pregnancy or triple test of the first trimester of pregnancy... The results of risk calculations obtained using the combined double test are much more accurate than risk calculations based on biochemical parameters alone or based on ultrasound alone.
If test results in the first trimester indicate a group at risk for fetal chromosomal abnormalities, the patient may be treated to rule out the diagnosis of chromosomal abnormalities. chorionic villus sampling.
During pregnancy 14 - 20 weeks by the last menstruation ( recommended time frame: 16-18 weeks) the following biochemical parameters are determined:
- α-fetoprotein (AFP)
- Inhibin A
Based on these indicators, the following risks are calculated:
- Down syndrome (trisomy 21)
- Edwards syndrome (trisomy 18)
- neural tube defects (spina bifida and anencephaly).
- Risk of trisomy on chromosome 13 (Patau syndrome)
- Triploidy of maternal origin
- Shereshevsky-Turner syndrome without dropsy
- Smith-Lemli-Opitz syndrome
- Corneli de Lange syndrome
This test is called quadruple test of the second trimester of pregnancy or quadruple biochemical screening in the second trimester of pregnancy... A truncated version of the test is the so-called triple or double tests of the second trimester, which includes 2 or indicators: hCG or free β-subunit of hCG, AFP, free estriol. It is clear that the accuracy of the double or double tests of the II trimester is lower than the accuracy of the quadruple test of the II trimester.
Another option for biochemical prenatal screening is biochemical screening for the risk of only neural tube defects in the second trimester of pregnancy... In this case, only one biochemical marker is determined: α-fetoprotein
When is the second trimester screening performed?
At 14 - 20 weeks of gestation. The optimal period is 16-18 weeks of pregnancy.
What is a quadruple test in the second trimester of pregnancy?
The main option for biochemical screening of the second trimester in the CIR is the so-called quadruple or quadruple test, when the determination of inhibin A is added to the determination of the three above-mentioned parameters.
Ultrasound screening in the first trimester of pregnancy.
In the first trimester of pregnancy, the main dimension used in calculating the risks is the width of the cervical translucency (English "nuchal translucency" (NT) ", French" clarté nuchale "). In Russian medical practice, this term is often translated as "collar space" (TVP) or "cervical fold". Cervical transparency, collar space and cervical fold are complete synonyms that can be found in different medical texts and mean the same thing.
Cervical transparency - definition
- Cervical transparency is what an ultrasound examination of the accumulation of subcutaneous fluid on the back of the fetus's neck looks like in the first trimester of pregnancy
- The term "cervical transparency" is used regardless of whether it contains septa or whether it is limited to the cervical region or surrounds the entire fetus.
- The frequency of chromosomal and other abnormalities is primarily associated with the width of the transparency, and not with how it looks as a whole.
- During the second trimester, the transparency usually resolves, but in some cases it can turn into either cervical edema or cystic hygromas with or without a combination with generalized edema.
Measurement of cervical transparency
Dates of pregnancy and coccygeal-parietal size
The optimal gestational age for measuring SP is between 11 weeks and 13 weeks 6 days. The minimum size of the CTE is 45 mm, the maximum is 84 mm.
There are two reasons for choosing 11 weeks as the earliest time to measure SHR:
- Screening requires the ability to perform a chorionic villus sampling before the time when this study can be complicated by cutting off the fetal limbs.
- On the other hand, many gross fetal defects can only be discovered after 11 weeks of gestation.
- The diagnosis of omphalocele is only possible after 12 weeks.
- Diagnosis of anencephaly is possible only after 11 weeks of pregnancy, since only from this time do ultrasound signs of ossification of the fetal skull appear.
- Evaluation of the four-chamber heart and large vessels is possible only after 10 weeks of pregnancy.
- The bladder is visualized in 50% of healthy fetuses at 10 weeks, in 80% at 11 weeks, and in all fetuses at 12 weeks.
Image and measurement
For measuring SHP ultrasound machine Must be of high resolution with video loop function and calibrators that can measure size to tenths of a millimeter. SP can be measured using an abdominal probe in 95% of cases, in cases where this is not possible, a vaginal probe should be used.
When measuring SHP, only the head and top part chest of the fetus. The magnification should be as large as possible, so that a slight offset of the markers results in a change in measurement of no more than 0.1 mm. When enlarging an image, before or after capturing the image, it is important to reduce the gain. This avoids measurement errors when the marker falls into the blurred area and thus the size of the NR will be underestimated.
A good sagittal section should be obtained, of the same quality as when measuring CTE. The measurement should be carried out in the neutral position of the fetal head: extension of the head can increase the TBP value by 0.6 mm, and flexion of the head can decrease the indicator by 0.4 mm.
It is important not to confuse the skin of the fetus and the amnion, since during these periods of pregnancy, both formations look like thin membranes. If in doubt, you should wait for the moment when the fetus makes a movement and moves away from the amnion. An alternative way is to ask the pregnant woman to cough or lightly tap on abdominal wall pregnant.
The largest perpendicular distance between the inner contours of the cervical transparency is measured (see figure below). Measurements are taken three times, for the calculation is used greatest value size. In 5-10% of cases, an entanglement of the umbilical cord around the fetal neck is found, which can significantly complicate the measurement. In such cases, 2 measurements are used: above and below the umbilical cord entanglement, the average value of these two measurements is used to calculate the risks.

End-of-trimester ultrasound scanning standards are being developed by the England-based Fetal Medicine Foundation (FMF). In the CIR group of companies, ultrasound is performed according to the FMF protocol.
Additional Ultrasound Signs of Down's Syndrome Risk
V recent times In addition to measuring SP, the following ultrasound signs are used to diagnose Down syndrome at the end of the first trimester of pregnancy:
- Definition of the nasal bone... At the end of the first trimester, the nasal bone not defined using ultrasound in 60-70% of fetuses with Down syndrome and only in 2% of healthy fetuses.
- Assessment of blood flow in the Arancian (venous) duct... Disturbances in the blood flow waveform in the duct arantia are found in 80% of fetuses with Down syndrome and only in 5% of chromosomally normal fetuses.
- Reducing the size of the maxillary bone
- An enlarged bladder (“megacystitis”)
- Moderate fetal tachycardia

The form of blood flow in the Arancian duct with Doppler. Above: norm; below: with trisomy 21.
Not only Down syndrome!
During an ultrasound scan at the end of the first trimester, an assessment of the fetal contour also reveals the following fetal abnormalities:
- Exencephaly - anencephaly
- Cystic hygroma (swelling at the level of the neck and back of the fetus), in more than half of cases due to chromosomal abnormalities
- Omphalocele and gastroschisis. The diagnosis of omphalocele can be made only after 12 weeks of pregnancy, since before this period, a physiological umbilical hernia, which is quite often detected, has no clinical significance.
- A single umbilical artery (in a large percentage of cases, it is combined with chromosomal abnormalities in the fetus)
How are risks calculated?
To calculate risks, special software is used. A simple determination of the level of indicators in the blood is not enough to decide whether the risk of developmental abnormalities is increased or not. The software must be certified for use for prenatal screening purposes. At the first stage of computer calculation, the figures of indicators obtained in laboratory diagnostics are converted into the so-called MoM (multiple of median, a multiple of the median), which characterize the degree of deviation of one or another indicator from the median. At the next stage of the calculation, the MoM is adjusted for various factors (body weight of a woman, race, the presence of certain diseases, smoking, multiple pregnancies, etc.). The result is the so-called adjusted MoM. In the third step of the calculation, the adjusted MoMs are used to calculate the risks. The software is specially tuned for the methods of determining indicators and reagents used in the laboratory. It is not acceptable to calculate risks using analyzes from another laboratory. The most accurate calculation of the risks of fetal anomalies is when using ultrasound data performed at 10-13 weeks of pregnancy.
What is MoM?
MoM is an English abbreviation of the term “multiple of median”, which means “multiple of median”. This is a coefficient showing the degree of deviation of the value of one or another indicator of prenatal screening from the average value for the gestational age (median). MoM is calculated using the following formula:
MoM = [The value of the indicator in the patient's blood serum] / [The value of the median indicator for the gestational age]
Since the indicator value and the median have the same unit of measure, the MoM value does not have a unit of measure. If the patient's MoM value is close to one, then the value of the indicator is close to the average in the population, if above one, it is above the average in the population, if below one, it is below the average in the population. With congenital malformations of the fetus, there may be statistically significant deviations in MoM markers. However, in pure form MoMs are almost never used in calculating the risks of fetal abnormalities. The fact is that in the presence of a number of factors, the average MoM values deviate from the population averages. These factors include the patient's body weight, smoking, race, pregnancy as a result of IVF, etc. Therefore, after obtaining the MoM values, the risk calculation program makes an adjustment for all these factors, as a result of which the so-called “corrected MoM value” is obtained. used in risk calculation formulas. Therefore, in the conclusion forms based on the analysis results, next to the absolute values of the indicators, the corrected MoM values for each indicator are indicated.
Typical MoM Profiles in Pregnancy Pathology
With various fetal anomalies, MoM values are combinedly deviated from the norm. Such combinations of MoM deviations are called MoM profiles for a particular pathology. The tables below show typical MoM profiles at different stages of pregnancy.
Typical MoM Profiles - First Trimester
Typical MoM Profiles - Second Trimester
Indications for prenatal screening of the 1st and 2nd trimester for the risk of fetal anomalies
Prenatal screening is now recommended for all pregnant women. The order of the Ministry of Health of the Russian Federation of 2000 obliges antenatal clinics conduct biochemical prenatal screening for all pregnant patients in the second trimester of pregnancy according to two indicators (AFP and hCG).
Order No. 457 of 28.12.2000 "On the improvement of prenatal diagnostics in the prevention of hereditary and congenital diseases in children ":
"At 16-20 weeks, take blood from all pregnant women for research at least two serum markers (AFP, hCG)"The importance of monitoring congenital diseases on an ongoing basis in Moscow is also considered in the decree of the Moscow government on the establishment of the city program "Children's Health" for 2003-2005.
"It is advisable to start in Moscow genetic monitoring of congenital malformations of newborns, prenatal screening for Down's disease and neural tube defects"On the other hand, prenatal screening should be completely voluntary. In most Western countries, it is the physician's responsibility to inform the patient about the feasibility of such tests and about the goals, possibilities and limitations of prenatal screening. The patient herself decides whether to do her tests or not. The CIR group of companies adheres to the same point of view. The main problem is that there is no cure for the detected anomalies. In case of confirmation of the presence of anomalies married couple is faced with a choice: to terminate the pregnancy or keep it. This is not an easy choice.
What is Edwards Syndrome?
This is a condition caused by the presence of an extra 18th chromosome in the karyotype (trisomy 18). The syndrome is characterized by gross physical abnormalities and mental retardation. This is a lethal condition: 50% of sick children die in the first 2 months of life, 95% - during the first year of life. Girls are affected 3-4 times more often than boys. The incidence in the population ranges from 1 case in 6,000 births to 1 case in 10,000 births (about 10 times less common than Down's syndrome).
What is the free β-subunit of hCG?
Molecules of a number of pituitary and placental hormones (thyroid-stimulating hormone (TSH), follicle-stimulating hormone (FSH), luteinizing hormone (LH) and human chorionic hormone (HCG)) have a similar structure and consist of α and β-subunits. The alpha subunits of these hormones are very similar and the main differences between the hormones are in the structure of the beta subunits. LH and hCG are very similar not only in the structure of the α-subunits, but also in the structure of the β-subunits. This is why they are hormones with the same effect. During pregnancy, LH production by the pituitary gland drops to almost zero, and hCG concentrations are very high. The placenta produces very large amounts of hCG, and although this hormone mainly enters the bloodstream in assembled(a dimeric molecule consisting of both subunits), a small amount of free (not bound to the α-subunit) β-subunit of hCG also enters the bloodstream. Its concentration in the blood is many times less than the concentration of total hCG, but this indicator can be much more reliable to indicate the risk of problems in an intrauterine fetus in early pregnancy. Determination of the free β-subunit of hCG in the blood is also important for the diagnosis of trophoblastic disease ( cystic skid and chorionepithelioma), some testicular tumors in men, monitoring the success of in vitro fertilization procedures.
Which indicator: total hCG or free β-subunit of hCG - is it preferable to use in the triple test of the second trimester?
The use of the determination of the free β-subunit of hCG in comparison with the determination of total hCG gives a more accurate calculation of the risk of Down syndrome, however, in the classical statistical calculations of the risk of Edwards syndrome in the population, the determination of the level of total hCG in the mother's blood was used. No such calculations were performed for the β-subunit of hCG. Therefore, a choice must be made between a more accurate calculation of the risk of Down syndrome (in the case of the β-subunit) and the possibility of calculating the risk of Edwards syndrome (in the case of total hCG). Recall that in the first trimester, to calculate the risk of Edwards syndrome, only the free β-subunit of hCG is used, but not the total hCG. Edwards syndrome is characterized by low numbers of all 3 indicators of the triple test, therefore similar cases you can do both variants of the triple test (with total hCG and with free β-subunit).
What is PAPP-A?
Pregnancy-associated plasma protein-A (PAPP-A) was first described in 1974 as a high-molecular-weight protein fraction in the serum of women in late pregnancy. It turned out to be a large zinc-containing metaloglycoprotein with a molecular weight of about 800 kDa. During pregnancy, PAPP-A is produced by syncytiotrophoblast (the tissue that is the outer layer of the placenta) and extravillous cytotrophoblast (islets of fetal cells in the thickness of the uterine lining) and enters the mother's bloodstream
The biological significance of this protein is not fully understood. It has been shown to bind heparin and is an inhibitor of granulocyte elastase (an enzyme inducible during inflammation), therefore it is assumed that PAPP-A modulates the immune response of the maternal organism and is one of the factors that ensures the development and survival of the placenta. In addition, it was found to be a protease that degrades protein 4, which binds insulin-like growth factor. Exists good reason believe that PAPP-A is one of the paracrine regulation factors not only in the placenta, but also in some other tissues, in particular in atherosclerotic plaques... It is proposed to use this marker as one of the risk factors ischemic disease hearts.
Maternal PAPP-A concentrations increase steadily with increasing gestational age. Greatest growth this indicator is observed at the end of pregnancy.
Over the past 15 years, PAPP-A has been studied as one of three risk markers for trisomy 21 (Down's syndrome) (along with free hCG β-subunit and collar space). It turned out that the level of this marker at the end of the first trimester of pregnancy (8-14 weeks) is significantly reduced in the presence of trisomy 21 or trisomy 18 in the fetus (Edwards syndrome). The uniqueness of this indicator is that its significance as a marker of Down's syndrome disappears after 14 weeks of pregnancy. In the second trimester, its levels in the maternal blood in the presence of trisomy 21 in the fetus do not differ from those in pregnant women with healthy fetus... If we consider PAPP-A as an isolated marker of the risk of Down syndrome in the first trimester of pregnancy, its definition at 8-9 weeks would be most significant. However, the free β-subunit of hCG is a stable marker of the risk of Down syndrome in the period of 10-18 weeks, i.e., later than PAPP-A. That's why optimal time donation of blood for a double test of the first trimester of pregnancy - 10-12 weeks.
The combination of measuring the level of PAPP-A with the determination of the concentration of the free β-subunit of hCG in the blood and the determination of TVP using ultrasound at the end of the first trimester of pregnancy makes it possible to identify up to 90% of women at risk of developing Down syndrome in the older age group (after 35 years). The likelihood of false positives is about 5%.
In addition to prenatal screening for the risk of Down syndrome and Edwards syndrome, the definition of PAPP-A is also used in obstetrics for the following types of pathology:
- The threat of miscarriage and stopping the development of pregnancy at a short time
- Cornelia de Lange syndrome.
Risk diagnostics stopping fetal development in early pregnancy was historically the first clinical application for the determination of PAPP-A in serum, proposed in the early 1980s. It has been shown that women with low levels PAPP-A in early pregnancy is at risk of further stopping the development of pregnancy and severe forms of late toxicosis... Therefore, it is recommended to determine this indicator within 7-8 weeks for women with a history of severe complications of pregnancy.
Cornelia de Lange syndrome- This is a rare form of congenital malformations of the fetus, found in 1 case in 40,000 births. The syndrome is characterized by mental and physical retardation, heart and limb defects, and characteristic features of facial features. It was shown that in this condition, the levels of PAPP-A in the blood in the period of 20-35 weeks are significantly lower than normal. A study by Aitken's group in 1999 showed that this marker can be used for screening for Cornelia de Lange syndrome in the second trimester of pregnancy, since the indicator levels in such pregnant women were, on average, 5 times lower than normal.
The reagents used to determine PAPP-A and the free β-subunit of hCG are orders of magnitude more expensive than the reagents used for most hormonal parameters, which makes this test more expensive than the determination of most hormones of the reproductive system.
What is α-fetoprotein?
It is a fetal glycoprotein produced first in the yolk sac, and then in the liver and gastrointestinal tract of the fetus. It is a transport protein in the fetal blood that binds a number of different factors (bilirubin, fatty acids, steroid hormones). It is a dual regulator of intrauterine growth. In an adult, AFP does not perform any known functions, although it can increase in the blood in liver diseases (cirrhosis, hepatitis) and in some tumors (hepatocellular carcinoma and germ cell carcinoma). In the mother's blood, the AFP level gradually increases with increasing gestational age and reaches a maximum by 30 weeks. AFP level in the mother's blood increases with defects in the neural tube in the fetus and with multiple pregnancies, decreases - with Down syndrome and Edwards syndrome.
What is Free Estriol?
Estriol is synthesized in the placenta from 16α-hydroxydehydroepianthrosterone sulfate from the fetus. The main source of estriol precursors is the fetal adrenal glands. Estriol is the main estrogenic hormone of pregnancy and is responsible for the growth of the uterus and preparation of the mammary glands for lactation.

90% of estriol after 20 weeks of gestation is derived from the DEA-C of the fetus. The high yield of DEA-C from the fetal adrenal gland is associated with low activity of 3β-hydroxysteroid dehydrogenase in the fetus. A protective mechanism that protects the fetus from excess androgenic activity is the rapid conjugation of steroids with sulfate. The fetus produces more than 200 mg of DEA-S per day, 10 times more than the mother. In the mother's liver, estriol is rapidly conjugated with acids, mainly with hyaluronic acid, and is thus inactivated. The most accurate method for determining the activity of the fetal adrenal glands is to determine the level of free (unconjugated) estriol.

Free estriol levels gradually increase as pregnancy progresses and can be used to diagnose fetal well-being in the third trimester of pregnancy. With a deterioration in the condition of the fetus in the third trimester of pregnancy, there may be a sharp drop in the level of free estriol. Free estriol levels are often low in Down syndrome and Edwards syndrome. Taking dexamethasone, prednisolone or metipred during pregnancy suppresses the function of the adrenal glands of the fetus, therefore the level of free estriol in such patients often decreases (decrease in the intake of estriol from the fetus). When taking antibiotics, the rate of conjugation of estriol in the mother's liver increases and the reabsorption of conjugates from the intestine decreases, so the level of estriol also decreases, but already due to the acceleration of its inactivation in the mother's body. For an accurate interpretation of the triple test data, it is very important that the patient provides a complete list of drugs taken or taken during pregnancy, with doses and timing of administration.
Algorithm for prenatal screening for the 1st and 2nd trimester of pregnancy.
1. We calculate the gestational age, preferably after consulting a doctor or with the help of a consultant.
Screening for the first trimester has its own characteristics. It is carried out in terms of 10-13 weeks of pregnancy and is rather strictly limited in terms of timing. If you donate blood too early or too late, if you make a mistake in calculating the timing of pregnancy at the time of donating blood, the accuracy of the calculation will decrease dramatically. Pregnancy in obstetrics is usually calculated on the first day of the last menstruation, although conception occurs on the day of ovulation, that is, with a 28-day cycle - 2 weeks after the first day of menstruation. Therefore, the terms of 10 - 13 weeks on the day of menstruation correspond to 8 - 11 weeks after conception.
To calculate the gestational age, we recommend using the obstetric calendar posted on our website. Difficulties in calculating the timing of pregnancy can be with irregular menstrual cycle, during pregnancy, which occurred soon after childbirth, with a cycle that deviates by more than a week from 28 days. Therefore, it is best to trust the professionals, and consult a doctor to calculate the timing of pregnancy, conduct an ultrasound scan and donate blood.
2. We do an ultrasound scan.
The next step should be an ultrasound scan within 10-13 weeks of pregnancy. The data from this study will be used by the risk calculation program in both the first and second trimester. It is necessary to start the examination with an ultrasound scan, since in the course of the study problems with the development of pregnancy (for example, a stop or delay in development), multiple pregnancies may be revealed, the timing of conception will be calculated quite accurately. The doctor performing the ultrasound will help the patient calculate the timing of blood donation for biochemical screening. If the ultrasound is done too early in the pregnancy, then the doctor may recommend repeating the study after some time.
To calculate the risks, the following data from the ultrasound report will be used: ultrasound date, coccygeal-parietal size (CTE) and collar space thickness (TVP) (English abbreviations CRL and NT, respectively), as well as visualization of the nasal bones.
3. We donate blood.
Having the results of an ultrasound scan and knowing the exact period of pregnancy, you can come to donate blood. Blood sampling for analysis for prenatal screening in the CIR group of companies is carried out daily, including weekends. V weekdays blood sampling is carried out from 7:45 to 21:00, on weekends and holidays: from 8:45 am to 5:00 pm. Blood sampling is performed 3-4 hours after the last meal.
During pregnancy 14 - 20 weeks after the last menstruation (recommended periods: 16-18 weeks), the following biochemical parameters are determined:
- Total hCG or free β-subunit of hCG
- α-fetoprotein (AFP)
- Free (unconjugated) estriol
- Inhibin A
4. We get the result.
Now you need to get the results of the analysis. The timing of the readiness of the results of the prenatal screening analysis in the CIR group of companies is one working day (except for the quadruple test). This means that tests taken from Monday to Friday will be ready on the same day, and those taken from Saturday to Sunday will be ready on Monday.
Conclusions based on the results of the study are issued to the patient in Russian.
Tibet. Explanations of terms and abbreviations
| Report date | Date of computer processing of results |
| Gestational age | Weeks + days |
| Date of ultrasound |  Date of ultrasound. Usually does not coincide with the date of blood donation. Date of ultrasound. Usually does not coincide with the date of blood donation. |
| Fruit | The number of fruits. 1 - singleton pregnancy; 2 - twins; 3 - triplets |
| ECO | Pregnancy resulted from IVF |
| CTE | Coccygeal-parietal size determined during ultrasound |
| MoM | Multiple of median, the degree of deviation of the result from the average for a given gestational age |
| Adj. MoM | Adjusted MoM. MoM value after correction for body weight, age, race, number of fetuses, diabetes, smoking, IVF infertility treatment. |
| NT | The thickness of the collar space (nuchal translucency). Synonym: cervical fold. In different versions of reports, either absolute values in mm or the degree of deviation from the median (MoM) can be given |
| Age risk | Average risk for this age group. No factors other than age are taken into account. |
| Tr. 21 | Trisomy 21, Down syndrome |
| Tr. eighteen | Trisomy 18, Edwards syndrome |
| Biochemical risk | The risk of fetal anomalies after computer processing of blood test data without taking into account ultrasound data |
| Combined risk | The risk of fetal anomalies after computer processing of blood test data, taking into account ultrasound data. The most accurate indicator of the degree of risk. |
| fb-HCG | Free β-subunit of hCG |
| PDM | Date of last menstruation |
| AFP | α-fetoprotein |
| HCG | Total HCG (human chorionic gonadotropin) |
| uE3 | Free estriol (unconjugated estriol) |
| + NT | The calculation was carried out taking into account the ultrasound data |
| mIU / ml | mIU / ml |
| ng / ml | ng / ml |
| IU / ml | IU / ml |
Additional Information.
Information for patients: Please note that if you plan to undergo prenatal screening in the CIR group of companies, then the data of ultrasound performed in other institutions will be taken into account only if there is a special agreement of the CIR group of companies with these institutions.
Information for doctors
Dear Colleagues! In accordance with Order of the Ministry of Health No. 457 and Resolution of the Moscow Government No. 572, the CIR group of companies provides services to other medical institutions for prenatal screening for the risk of chromosomal abnormalities. You can invite our staff to come to you with a lecture on this program. To refer a patient for screening, the attending physician must complete a special referral. The patient can come to donate blood on her own, but it is also possible to take blood in other institutions with subsequent delivery to our laboratory, including by our courier. If you want to receive the results of double, triple and quadruple tests of the first and second trimesters of pregnancy, combined with ultrasound data, the patient must come to us for an ultrasound scan, or we must sign a special agreement with your institution and include your ultrasound specialists in the program, but only after visit of our expert in functional diagnostics to your institution and get acquainted with the quality of the equipment and the qualifications of specialists.